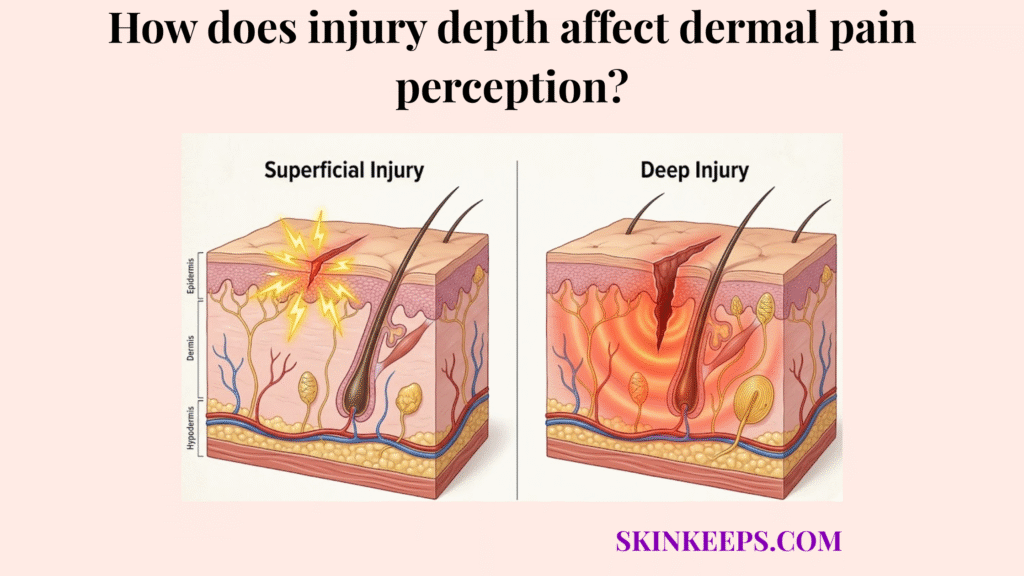
Injury depth affects dermal pain perception because different skin depths contain different densities and exposure patterns of sensory endings, so shallow injuries often produce sharp stinging pain while deeper injuries more often produce duller, heavier, or throbbing pain.
A simple paper cut or a superficial abrasion can feel far more agonizingly sharp than a deeper bruise or a narrow puncture. This is because the skin’s biological alarm system places its most reactive, fast-firing sensors right at the surface. When those sensors are exposed to the air without being destroyed, they generate an intense, continuous sting.
Understanding how injury depth affects dermal pain perception requires mapping this biological baseline, exploring how superficial exposure amplifies the signal, tracing deep tissue involvement, comparing common wound types, and matching clinical treatments to the specific pain signature.
What is the biological baseline for how injury depth affects dermal pain perception?
The biological baseline for how injury depth affects dermal pain perception is the nociceptor gradient: pain begins when free nerve endings and nociceptors detect damage, but the density, exposure, and signal quality of those endings change across skin depth.
Nociceptors are specialized pain-detecting free nerve endings distributed throughout the skin. They convert thermal, chemical, or mechanical damage into the electrical signals that the brain registers as pain.
The skin does not use one generic alarm wire. It relies on a gradient, shifting from fast-firing networks near the surface to slower, ache-producing networks in the deep tissue.
Pain-pathway references identify 2 major nociceptive fiber types: A-delta fibers and C fibers. A-delta fibers are associated with the first sharp, fast pain signal, while C fibers are associated with slower, burning, aching, or lingering pain. That two-fiber distinction is the clearest quantitative foundation for explaining how injury depth changes pain quality and which receptors transmit sharp vs dull pain in the dermis (Kendroud et al., 2022).
How does superficial exposure explain how injury depth affects dermal pain perception?
Superficial exposure explains how injury depth affects dermal pain perception because shallow wounds breach the epidermal barrier and leave upper-level pain endings vulnerable to air, movement, temperature shifts, and surface irritation.
A shallow cut or scrape removes the dead cells of the stratum corneum but leaves the living papillary dermis beneath it largely intact. The nerve endings housed there are not destroyed; they are stripped of their insulation. This breach not only exposes nerves but also explains how barrier disruption increases TEWL, leading to rapid surface dehydration.
This creates a state of continuous overstimulation. The raw, exposed nerve endings react violently to minor drafts, sweat, or clothing friction, generating the intense, sharp stinging pain characteristic of superficial injury.
Burn-depth literature gives the strongest natural proof. Superficial partial-thickness burns are described as very painful and generally heal in about 10 to 15 days, whereas deep partial-thickness burns can be less painful because nerves are more damaged and usually heal over 3 to 5 weeks. That contrast shows that pain intensity and visible depth do not scale in a simple straight line (Walker et al., 2023).
How does deep tissue involvement influence how injury depth affects dermal pain perception?
Deep tissue involvement influences how injury depth affects dermal pain perception by shifting the dominant signal away from exposed superficial sting and toward deeper pressure, tissue strain, inflammation, or aching pain.
When an injury penetrates through the reticular dermis and into the hypodermis (subcutaneous fat), it bypasses the dense concentration of superficial A-delta fibers. Instead, the trauma engages the sparser, deeper C fibers.
Because these deeper structures are sheltered beneath the tissue, they are not exposed to air or surface friction. Therefore, the pain they generate is driven by internal tissue swelling, physical stretching from inflammation, and vascular throbbing.
This is why deep pain is often felt as a heavy, poorly localized ache rather than a sharp, easily pinpointed sting.
How does nerve density explain how injury depth affects dermal pain perception across skin layers?
Nerve density explains how injury depth affects dermal pain perception because the skin’s highest-priority alarm signaling is concentrated closer to the surface, where shallow injury can activate more nearby pain endings at once.
The skin distributes its sensory receptors unevenly to maximize efficiency. It places the vast majority of its fast-acting, high-resolution alarm sensors right beneath the surface to catch environmental threats immediately.
If you combine a shallow depth with a high-density body region—like the fingertips or lips—the result is massive local nociceptor activation. This perfectly aligns with how receptor density varies across dermal regions of the body, dictating where pain feels most intense. This creates a spatial summation effect, where the brain receives hundreds of sharp pain signals from a very tiny, shallow area.
How do various wounds compare regarding how injury depth affects dermal pain perception?
Various wounds compare differently because injury depth affects dermal pain perception by changing whether the dominant signal comes from exposed superficial nociceptors or from deeper pressure and inflammatory pathways. This structural difference perfectly explains why certain skin injuries produce more pain than others despite appearing less dangerous on the surface.
A simple abrasion scrapes the surface, setting off a widespread, burning, A-delta firestorm. A bruise leaves the surface entirely intact but crushes the deep vasculature, triggering a dull, inflammatory C-fiber ache over several days.
A puncture wound creates a narrow but deep channel. The initial entry stings sharply, but the lingering pain shifts rapidly to a deep, localized throb as the internal tissues swell.
| Injury type | Primary depth | Pain quality | Pain persistence |
|---|---|---|---|
| Paper cut | Very superficial | Sharp, stinging | Often persistent |
| Abrasion | Superficial broad injury | Burning, raw | Often prolonged |
| Burn | Superficial to variable | Burning, searing | Can stay intense |
| Puncture | Narrow, deeper entry | Deep, localized, duller initially | Variable |
| Bruise | Deeper tissue involvement | Aching, pressure-like, throbbing | Often delayed and lingering |
How do full-thickness and deeper injuries change how injury depth affects dermal pain perception?
Full-thickness and deeper injuries change how injury depth affects dermal pain perception because greater structural damage can reduce sharp superficial signaling while increasing deeper inflammatory, pressure-like, or delayed pain.
It is a biological paradox: more severe depth does not always equal sharper immediate pain. When trauma is profound enough to destroy the reticular dermis, it incinerates or slices through the very nociceptors required to send the alarm signal.
This means the center of a catastrophic wound may be physically numb, while the less-damaged, shallower edges of the wound scream in agony.
What clinical strategies manage cases where injury depth affects dermal pain perception?
Clinical strategies manage cases where injury depth affects dermal pain perception best when treatment matches the wound’s pain signature instead of treating all wounds the same way.
You cannot treat a raw, stinging scrape with the same logic you use to treat a deep, aching bruise. The biological source of the pain is entirely different.
How does sealing shallow wounds help when injury depth affects dermal pain perception?
Sealing shallow wounds helps when injury depth affects dermal pain perception because occlusive or moist coverage reduces air exposure, friction, and repeated stimulation of exposed superficial nerve endings.
By applying a physical barrier like a hydrocolloid dressing, you replace the missing epidermis. This physically insulates the raw A-delta fibers, shutting down the continuous stinging loop immediately.
A hydrocolloid review reported that one acute-wound comparison found 91% pain-free outcomes with hydrocolloid treatment versus 30% with conventional treatment, alongside shorter healing in that study (Thomas, 2008).
How do deeper-pain strategies help when injury depth affects dermal pain perception?
Deeper-pain strategies help when injury depth affects dermal pain perception because deeper injuries are less about exposed surface nerves and more about tissue stress, swelling, and inflammatory pain.
For deep punctures, severe bruises, or sprains, topical surface barriers will not stop the pain because the surface nerves are not the issue. These injuries require anti-inflammatory support, rest, elevation, and appropriate compression to reduce the deep tissue swelling that triggers the C-fiber ache.
Pain Management Pathway
- Problem → wound depth changes the pain signature.
- Implication → shallow injuries sting; deeper injuries ache or throb.
- Solution → insulate exposed superficial wounds and manage deeper inflammatory pain differently.
What are the key takeaways for how injury depth affects dermal pain perception?
The key takeaways are that injury depth affects dermal pain perception because nerve density is highest near the surface, superficial exposure sharpens pain, and deeper tissue involvement shifts pain into a different sensory register.
Summary Checklist
What steps can you take to treat wounds where injury depth affects dermal pain perception?
Wounds are treated most effectively when injury depth affects dermal pain perception in a recognizable way and first aid is matched to that pattern early.
Final Execution Checklist
Quick Answers About How Injury Depth Affects Dermal Pain Perception
Why can a paper cut hurt more than a deeper wound?
A paper cut can hurt more because it breaches the epidermis to expose a high density of superficial A-delta pain fibers to the air. The shallow depth leaves these nerves raw and repeatedly stimulated without destroying them.
Why do shallow wounds sting more sharply?
Shallow wounds sting sharply because they trigger the fast-firing, myelinated A-delta fibers located in the upper papillary dermis. These nociceptors are designed to send an immediate, bright alarm signal upon environmental exposure.
What is the nociceptor gradient in the skin?
The nociceptor gradient describes the shift in pain-sensor distribution from the surface down to the deep tissue. The skin places its fastest, most sensitive alarm receptors near the surface and relies on duller, pressure-sensitive receptors in the deeper layers.
Do deeper injuries always hurt more?
No. Deeper injuries often destroy the high-density superficial nerve endings entirely, muting the sharp stinging response. The pain then shifts to a deeper, duller ache driven by tissue stress and inflammation rather than raw exposure.
Why do burns change pain with depth?
Superficial burns leave nerve endings alive, exposed, and intensely irritated, resulting in agonizing pain. Full-thickness burns destroy these nerve endings completely, blocking the pain signal and making the deepest part of the wound physically numb.
What kind of dressing helps shallow stinging wounds?
Occlusive coverage, such as a hydrocolloid dressing, helps shallow stinging wounds by replacing the broken epidermal seal. This insulates the exposed nerve endings from air, friction, and environmental temperature shifts, rapidly stopping the stinging.
Why does deeper pain feel duller or heavier?
Deeper pain feels duller because it is primarily transmitted by slow, unmyelinated C fibers located in the reticular dermis and hypodermis. These fibers respond to broad tissue strain, swelling, and inflammation rather than sharp surface contact.
Conclusion
In conclusion, injury depth affects dermal pain perception because the skin’s alarm system is layered, with dense superficial nociceptors driving sharp exposed pain and deeper tissues more often producing duller, heavier, or inflammatory pain.
By mapping the nociceptor gradient, we demystify the pain paradox: visual severity does not dictate pain intensity. A shallow scrape leaves the nerves screaming, while a catastrophic deep puncture may silence the primary alarm entirely. Matching our first aid response to this exact depth-specific pain signature allows us to effectively calm the biological fire where it actually burns.