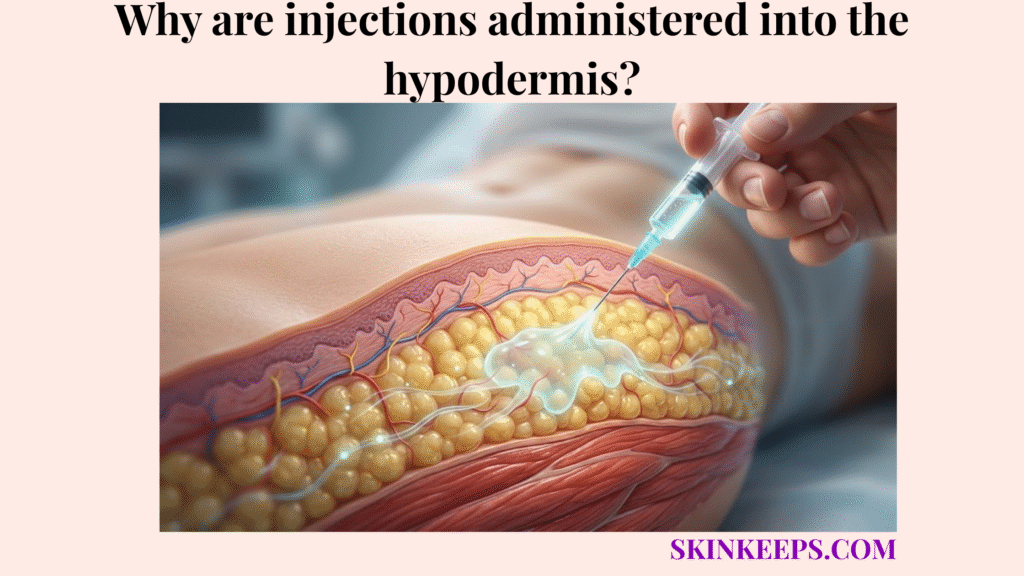
Injections are administered into the hypodermis when a medication is designed for subcutaneous tissue delivery because this layer can hold small medication volumes and release them into circulation more gradually than muscle or blood vessels. This slow absorption profile makes it the clinical standard for drugs that require sustained physiological effects.
This guide explains the anatomical and pharmacokinetic reasons behind hypodermal administration, covering medication types, depth errors, lipohypertrophy, and injection technique. Readers must always follow their clinician’s instructions and the specific medication labeling, using this safety checklist solely as an educational supplement.
What anatomical features make subcutaneous tissue useful for drug administration?
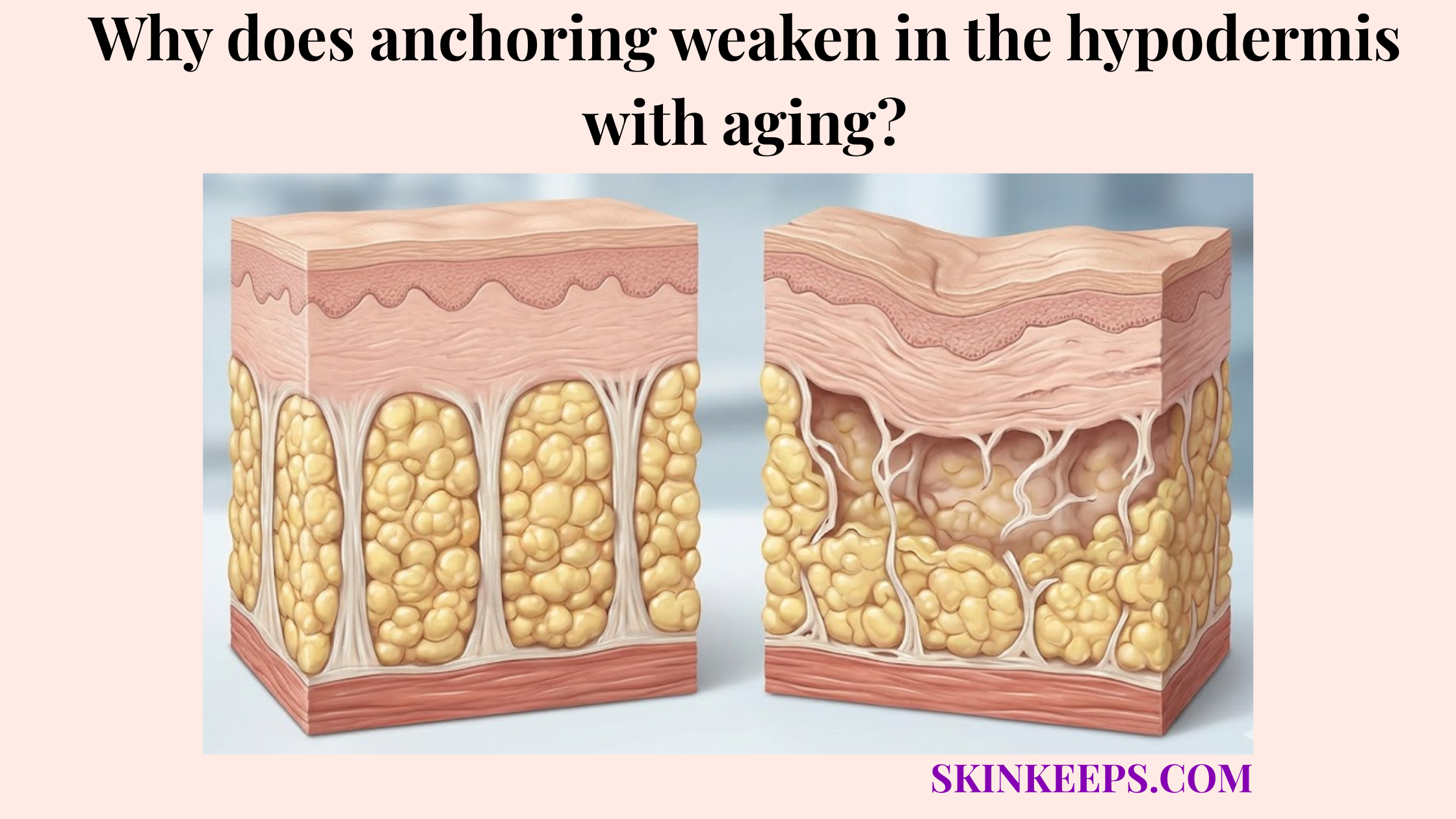
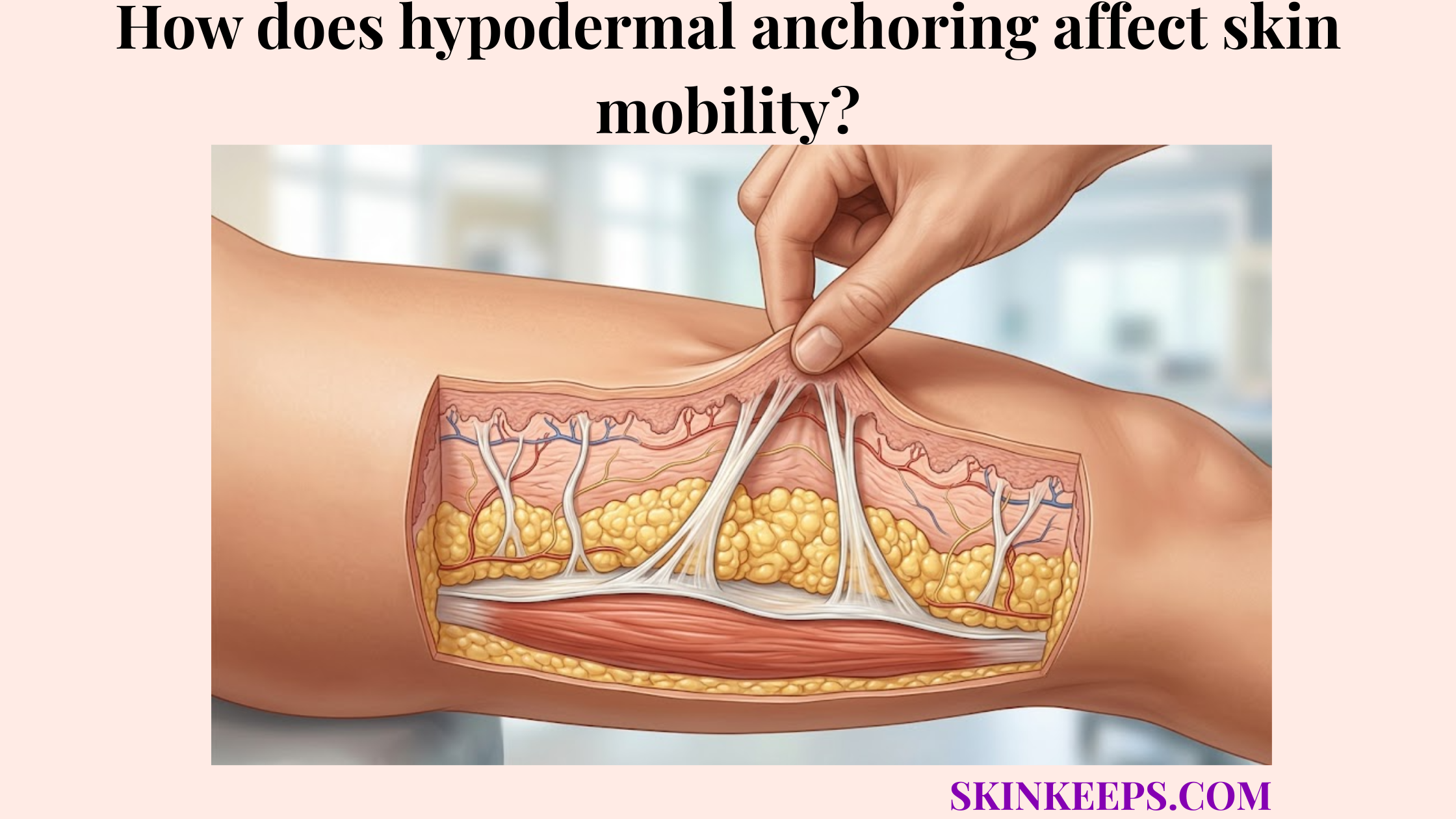
Subcutaneous tissue is useful for drug administration because it contains adipose tissue beneath the dermis that can hold selected medication volumes and allow gradual uptake through local blood vessels. Because the hypodermis supports adipose storage, insulation, and structural anchoring, it functions as a highly compliant, fatty tissue compartment.
This distinct biological environment allows the tissue to accept safely administered fluids without generating excessive internal tension.
How does adipose tissue accommodate small injection volumes?
Adipose tissue accommodates small injection volumes by providing a soft subcutaneous compartment where medication can form a local depot before gradual absorption. These fat lobules are separated by flexible connective walls that gently yield to accommodate the introduced fluid.
Some pediatric clinical guidance lists 1.5 mL as a recommended subcutaneous injection volume at several sites and notes that larger abdominal-wall volumes such as 3 mL may be tolerated in selected contexts, so the article must frame injection volume as medication- and protocol-specific. [Royal Children’s Hospital Melbourne]
How does lower sensory density affect injection comfort?
Lower sensory density may affect injection comfort because subcutaneous tissue is generally less densely innervated than the superficial dermis, but pain still depends on needle, medication, technique, and individual sensitivity. The dermis contains a rich network of sensory nerves designed to detect touch and sharp pain.
By delivering medication past the dermis into the hypodermis, a properly executed subcutaneous injection may reduce sharp discomfort, though it is not entirely pain-free.
How does the hypodermal vascular network regulate medication absorption rates?
The vascular network regulates medication absorption rates by controlling how quickly medication moves from the subcutaneous depot into nearby capillaries and then into systemic circulation. Understanding this blood flow supports hypodermal heat retention and explains fundamental pharmacokinetics.
Because the hypodermis is often less vascularized than skeletal muscle, it generally offers a slower, more sustained systemic drug delivery profile.
How does subcutaneous tissue create sustained absorption?
Subcutaneous tissue can create sustained absorption because medication must diffuse through local tissue fluid and enter the local capillary network before reaching systemic circulation. This physiological barrier prevents the immediate, rapid systemic entry seen in intravenous administration.
By trapping the drug temporarily in a fatty medication depot, the body naturally meters out the dose over hours or days.
How do temperature, exercise, and perfusion affect absorption?
Temperature, exercise, and local perfusion can affect absorption because warmer tissue, increased local blood flow, or active nearby muscle can change how quickly medication leaves the injection site. Applying heat or vigorously exercising the injected limb may increase local capillary uptake, potentially accelerating the drug’s systemic entry.
Patients should always follow clinical guidance regarding exercise timing and site selection to maintain predictable medication levels.
| Tissue Layer | Vascular Density | Typical Absorption Pattern | Clinical Meaning |
|---|---|---|---|
| Dermis | Rich superficial vessels and nerves | Small-volume intradermal use only | Wrong depth can cause pain, wheal, or poor drug delivery |
| Hypodermis / subcutaneous tissue | Moderate/local capillary uptake through fat | Gradual depot-style absorption for selected medications | Useful for insulin, LMWH, GLP-1 drugs, and some biologics |
| Skeletal muscle | Higher perfusion than fat | Faster uptake for many drugs | Accidental IM insulin delivery may increase hypoglycemia risk |
| Intravenous route | Direct blood access | Immediate systemic delivery | Used for drugs requiring direct bloodstream administration |
Which medications require or commonly use delivery into the deep fatty layer?
Medications require or commonly use delivery into the deep fatty layer when their formulation is designed for subcutaneous absorption, gradual systemic uptake, or patient-administered injection under clinical instruction. A hypodermal injection provides a safe, highly accessible route for self-administration.
However, medication efficacy depends entirely on adhering to the exact tissue layer intended by the manufacturer’s pharmaceutical design.
Why are insulin and GLP-1 drugs commonly injected subcutaneously?
Insulin and many GLP-1 receptor agonists are commonly injected subcutaneously because their formulations are designed for absorption through the subcutaneous tissue rather than digestion through the gastrointestinal tract. Basal insulin relies on the slow-release properties of the fat layer to mimic background physiological levels, while rapid-acting insulin requires precise meal-time coordination.
Similarly, many modern peptide biologics and metabolic therapies utilize this pathway to bypass the stomach and ensure systemic availability.
Why are heparin and enoxaparin administered subcutaneously?
Heparin and enoxaparin may be administered subcutaneously because low-molecular-weight heparin therapy is often designed for predictable absorption from the subcutaneous layer under prescribed protocols. These potent anticoagulants require steady physiological delivery to manage clotting risks effectively.
UConn Health’s patient guide states that enoxaparin is injected subcutaneously into the right or left abdomen at least 2 inches from the belly button, while Sanofi’s Clexane guide uses at least 5 cm from the umbilicus in its administration instructions. [UConn Health] and [Sanofi]
| Medication / Drug Class | Why Subcutaneous Route Is Used | Key Safety Note |
|---|---|---|
| Insulin | Designed for absorption through subcutaneous tissue | Wrong depth can alter absorption and glucose response |
| Basal insulin | Gradual absorption supports longer action profile | Do not inject into muscle or lipohypertrophy |
| Rapid-acting insulin | Subcutaneous absorption supports mealtime use when prescribed | Exercise, heat, and site can affect absorption |
| Enoxaparin / LMWH | Designed for SC anticoagulant administration | Bruising/bleeding precautions matter |
| GLP-1 receptor agonists | Injectable peptide-based metabolic therapy | Follow device-specific instructions |
| Biologics | Some are formulated for SC self-administration | Route and site depend on product labeling |
| Fertility hormones | Some are SC under prescribed protocols | Technique and timing are clinician-directed |
Why can injecting outside the subcutaneous fat compartment cause adverse reactions?
Injecting outside the subcutaneous fat compartment can cause adverse reactions because medication absorption, pain, tissue reaction, and safety profile change when the drug enters the dermis or muscle instead of the intended hypodermal layer. Every medication is pharmacokinetically calibrated for a specific tissue density.
Missing the target depth alters how quickly the drug enters the bloodstream, potentially triggering unintended physiological responses.
Why can accidental intramuscular injection be risky?
Accidental intramuscular injection can be risky because skeletal muscle has higher perfusion than subcutaneous fat, so some medications may absorb faster than intended. Muscle tissue is highly vascularized to support intense physical activity.
For example, if insulin is mistakenly injected into muscle, the rapid absorption can significantly increase the risk of unexpected hypoglycemia.
Why can intradermal or too-shallow injection cause local reactions?
Intradermal injection or too-shallow placement can cause local reactions because the dermis is denser, more sensitive, and less suited for many medications intended for subcutaneous delivery. Delivering fluid into this tightly packed collagen network often results in a painful raised wheal or surface leakage.
Depending on the medication, this shallow placement may also cause poor absorption or significant local tissue irritation.
| Error Type | Tissue Hit | Mechanism | Possible Clinical Effect |
|---|---|---|---|
| Too shallow | Dermis | Dense, sensitive tissue not intended for many SC drugs | Pain, swelling, leakage, poor absorption |
| Correct depth | Hypodermis | Depot-style absorption through local capillaries | Intended absorption profile |
| Too deep | Muscle | Higher perfusion and muscle activity | Faster absorption for some drugs, especially insulin |
| Same site repeatedly | Damaged adipose tissue | Local tissue hypertrophy or scarring | Erratic absorption |
| Bruised/infected site | Abnormal tissue | Local inflammation or bleeding risk | Pain, poor absorption, complications |
How does repeated localized hypodermal injection cause lipohypertrophy?
Repeated localized hypodermal injection can cause lipohypertrophy when frequent injections, poor site rotation, needle reuse, or repeated insulin exposure alter the subcutaneous fat tissue. These chronic biological stressors disturb the local tissue architecture, leading to undesirable physical changes.
Recognizing and avoiding these abnormal tissue patches is a critical component of injection safety and glycemic management.
How does repeated insulin exposure alter local fat tissue?
Repeated insulin exposure can alter local fat tissue because insulin has anabolic effects, and repeated injections into the same area can encourage thickened or rubbery subcutaneous tissue changes. As the hormone concentrates in one spot, it may stimulate local adipocytes and fibrous septa connect layers in the hypodermis to thicken abnormally.
TREND Diabetes describes lipohypertrophy as a thickened, rubbery lesion of fat tissue in the subcutaneous layer and states it is found in at least 2/3 of patients who use insulin in that guidance. [TREND Diabetes]
Why does injecting into lipohypertrophy distort absorption?
Injecting into lipohypertrophy can distort absorption because thickened subcutaneous tissue does not absorb insulin as predictably as healthy rotated injection sites. The disorganized, altered fat limits the medication’s ability to enter the capillary network smoothly.
TREND Diabetes cites injection-technique data in which 39.1% of people experienced unexplained hypoglycaemia and 49.1% experienced glycaemic variation in the referenced insulin-injection context, so the writer must frame lipohypertrophy as a glycemic-variability risk rather than a cosmetic lump. [TREND Diabetes]
What physical technique helps target the subcutaneous lipid matrix safely?
Physical technique helps target the subcutaneous lipid matrix safely by matching site selection, needle length, needle angle, skin-fold use, and injection depth to the medication, device, and patient’s tissue thickness. General education supports these techniques, but patients must always defer to their personal clinical training.
There is no one-size-fits-all injection method, as specific medications demand specific delivery protocols.
When is the pinch technique useful?
The pinch technique is useful when a skin fold helps lift subcutaneous tissue away from muscle and reduce the risk of injecting too deeply. By elevating the fat layer, the needle is far less likely to penetrate the highly vascular skeletal muscle beneath.
For enoxaparin/Clexane examples, UConn Health instructs patients to pinch 1 inch of cleaned abdominal skin and insert the needle at a 90° angle, while Sanofi’s Clexane guide says the full needle is introduced vertically at a 90° angle into the skin fold. [UConn Health] and [Sanofi]
How should needle angle and needle length be chosen?
Needle angle and needle length should be chosen according to the medication device, prescribed instructions, body habitus, injection site, and clinician training. Because hypodermal fat decreases with age and varies widely by patient, depth controls must be continuously evaluated by a healthcare professional.
FITTER guidance states that 4–5 mm pen needles generally do not need a skin lift in most cases, 6 mm and longer needles commonly need a skin lift, and a 90° injection is recommended in that guide; other FIT Canada guidance notes that lean individuals using longer needles may need a 45° angle to reduce possible intramuscular injection risk. [Forum for Injection Technique]
| Technique Factor | Why It Matters | Safe Writer Language |
|---|---|---|
| Medication type | Different drugs have different route requirements | Follow prescribed route and label |
| Needle length | Controls depth and IM risk | Choose with clinician/device guidance |
| Needle angle | Affects depth relative to tissue thickness | Protocol-specific; not one-size-fits-all |
| Skin fold | May lift fat away from muscle | Useful in selected contexts |
| Injection site | Affects absorption and tissue risk | Rotate and avoid damaged tissue |
| Site condition | Bruising, hard lumps, redness, infection can affect safety | Inspect before injecting |
| Sharps disposal | Prevents needle-stick injury | Use approved sharps container |
What daily checklist supports safe hypodermal medication delivery?
A daily checklist supports safe hypodermal medication delivery by combining site inspection, correct device use, site rotation, tissue protection, and clinician-guided response to complications. Developing a consistent routine limits accidental depth errors and mitigates localized tissue trauma.
Prioritizing safe practices preserves the hypodermis as a viable and healthy drug delivery site.
How should site rotation and tissue care be handled?
Site rotation and tissue care should be handled by moving injections through appropriate areas, avoiding damaged tissue, and checking for hard lumps, bruising, redness, swelling, or infection before injecting. Consistently altering the injection location helps prevent lipohypertrophy and localized scarring.
RCH guidance advises avoiding skin that is edematous, bruised, hard, red, broken, infected, over bony areas, or where clothing may rub, while UConn’s enoxaparin guide recommends rotating abdominal injection sites and alternating left and right sides. [Royal Children’s Hospital Melbourne] and [UConn Health]
What administration protocol keeps injection practice safer?
A safer administration protocol keeps injection practice aligned with the prescription by confirming the medication, dose, device, site, technique, and disposal method before each injection. Verifying these elements ensures the drug enters the correct tissue layer using the manufacturer’s approved methodology.
For Clexane/enoxaparin, Sanofi’s guide instructs users not to rub the injection site after administration and to dispose of the used syringe in a sharps container after injection; UConn’s guide also includes sharps disposal and bleeding-warning instructions. [Sanofi] and [UConn Health]
Daily Hypodermal Injection Safety & Site Rotation Checklist
FAQs About Injections Administered Into the Hypodermis
Why are some injections given into the hypodermis?
Some injections are given into the hypodermis because subcutaneous tissue can hold selected medications and release them gradually through local blood vessels. This route is useful only for medications formulated and prescribed for subcutaneous administration.
Is subcutaneous injection the same as intramuscular injection?
No. Subcutaneous injection places medication into the fat layer beneath the dermis, while intramuscular injection places medication into muscle. The route matters because muscle is usually more vascular, so some drugs may absorb faster if injected too deeply.
Which medications are commonly injected subcutaneously?
Common subcutaneous medications include insulin, some GLP-1 receptor agonists, some biologics, fertility hormones, and anticoagulants such as enoxaparin. Each drug must be given exactly as prescribed because route, site, dose, and device instructions vary.
Why can intramuscular insulin injection be dangerous?
Intramuscular insulin injection can be risky because insulin may absorb faster from muscle than from subcutaneous fat. Faster absorption can increase the risk of unexpected hypoglycemia, especially if the insulin was intended for subcutaneous delivery.
What is lipohypertrophy?
Lipohypertrophy is a thickened or rubbery change in subcutaneous fat that can develop after repeated insulin injections into the same area. TREND Diabetes guidance describes lipohypertrophy as affecting at least 2/3 of insulin users in that guidance context.
Should every subcutaneous injection use a pinch and 90-degree angle?
No. Pinch technique and angle depend on medication, device, needle length, site, tissue thickness, and clinician guidance. Some enoxaparin instructions use a skin fold and 90° angle, while insulin needle guidance may differ by needle length and patient factors.
When should someone call a clinician after a subcutaneous injection?
A clinician should be contacted for severe or spreading redness, warmth, drainage, fever, excessive bruising, bleeding that will not stop, unexpected blood glucose swings, hard injection-site lumps, or symptoms that feel unusual after the medication.
Conclusion
Injections are administered into the hypodermis when a medication is designed for subcutaneous delivery and needs controlled absorption through the adipose-rich layer beneath the dermis. This route depends on correct site selection, tissue depth, medication formulation, and trained technique.
At SkinKeeps, we explain skin structure through evidence-based dermatology, pharmacology, and anatomy. Understanding subcutaneous injection anatomy helps readers respect why medication route, depth, rotation, and clinician guidance matter for safe tissue-specific delivery.