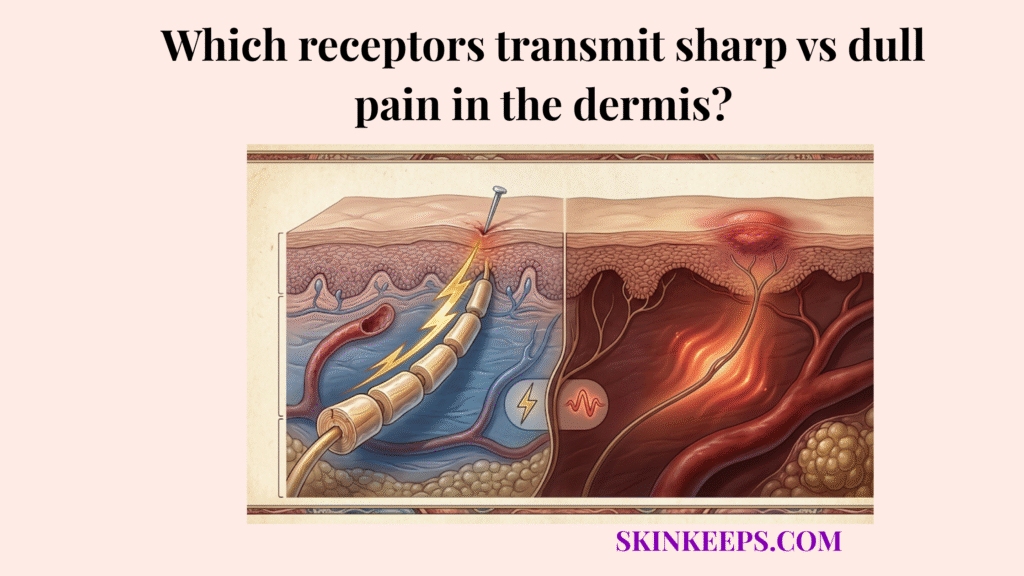
Receptors transmit sharp vs. dull pain through two main nerve-fiber pathways: A-delta fibers, which carry fast, sharp, well-localized pain, and C-fibers, which carry slower, duller, burning, or aching pain.
Pain is not carried at one speed or in one form. The nervous system uses dual channels to separate the immediate, electrical shock of an injury from the lingering ache that ensures you protect the tissue while it heals.
Understanding how receptors transmit sharp vs. dull pain makes it easier to trace the baseline biology, examine how myelination changes conduction speed, track the injury-triggered two-step response, compare the fibers, and match treatment logic to the specific pathway.
What is the biological baseline for how receptors transmit sharp vs. dull pain?
The biological baseline for how receptors transmit sharp vs. dull pain is that nociceptors detect noxious stimuli and relay those signals through 2 major afferent fiber systems: A-delta fibers and C-fibers. (Kendroud et al., 2022)
Nociceptors function as specialized free nerve endings that exclusively detect harmful mechanical, thermal, or chemical stimuli. When triggered, they route the alarm into dual pathways rather than a single generic channel.
The body benefits immensely from this split: an immediate, fast alarm forces a protective reflex, while a slower, sustained signal ensures the tissue remains guarded during recovery.
Pain-pathway references identify 2 major nociceptive fiber types: A-delta fibers and C-fibers. A-delta fibers are lightly myelinated and associated with initial sharp pain, while C-fibers are unmyelinated and associated with slower dull, burning, or aching pain (Armstrong et al., 2023). This two-fiber distinction is the clearest quantitative foundation for the whole topic.
How does myelination determine how receptors transmit sharp vs. dull pain?
Myelination determines how receptors transmit sharp vs. dull pain because A-delta fibers are myelinated and conduct faster, while C-fibers are unmyelinated and conduct more slowly.
Myelination provides an insulating lipid wrapping around the nerve axon that prevents electrical signal leakage. This insulation enables saltatory conduction, a rapid signaling process where the electrical impulse jumps between uninsulated gaps (nodes) along the fiber rather than traveling the entire continuous length.
This structural difference creates 2 distinct conduction classes within the nervous system. Myelinated fast-conducting pain fibers (A-delta) use this jumping mechanism to deliver signals in milliseconds, whereas unmyelinated slow-conducting pain fibers (C-fibers) must transmit the signal continuously along the entire fiber membrane (Arcilla et al., 2023).
How does injury trigger how receptors transmit sharp vs. dull pain?
Injury triggers how receptors transmit sharp vs. dull pain by activating nociceptors in a two-step sequence: a fast A-delta-mediated first pain followed by a slower C-fiber-mediated second pain.
When superficial dermal nerve endings are more reactive during an injury, the immediate, bright sting you feel is the first pain arriving instantly. Seconds later, a heavy, throbbing ache sets in, which is the second pain arriving after the slower signal finally reaches the brain.
Both waves belong to the exact same injury event, separated entirely by the physical travel time of the dual-stage pain response.
Experimental and review literature consistently distinguishes these as 2 separate temporal phases, with myelinated fibers dominating the first and C-fibers dominating the second (Basbaum et al., 2009).
How do A-delta and C-fibers compare in how receptors transmit sharp vs. dull pain?
A-delta and C-fibers compare differently because receptors transmit sharp vs. dull pain through pathways that differ in speed, myelination, localization, and sensory quality.
A-delta fibers structurally feature a thin myelin sheath that enables rapid, highly targeted communication. C-fibers lack this myelin sheath entirely, resulting in a primitive, slow transmission network.
Behaviorally, the fast fibers trigger an immediate warning to pull away from danger, while the slow fibers generate a lingering protective pain that forces you to rest the damaged area.
| Fiber type | Pain quality | Signal speed | Fiber structure | Main function |
|---|---|---|---|---|
| A-delta fibers | Sharp, prickly, well localized | Fast | Myelinated | Immediate danger alert |
| C-fibers | Dull, burning, aching, diffuse | Slow | Unmyelinated | Ongoing protection and behavioral avoidance |
How do fast and slow pain signals differ when receptors transmit sharp vs. dull pain?
Fast and slow pain signals differ when receptors transmit sharp vs. dull pain because sharp A-delta signaling is usually more precisely localized, while slower C-fiber signaling is broader, heavier, and more persistent.
A sharp localized pain signal tells the brain exactly where the skin was breached, allowing for precise defensive action. You know exactly where a needle pierced the skin.
A dull burning aching pain signal diffuses across a wider area, creating a generalized zone of discomfort that is harder to pinpoint with one finger. This broader signaling perfectly illustrates how injury depth affects dermal pain perception, ensuring the entire region is protected while the tissue heals.
What treatments manage the distinct ways that receptors transmit sharp vs. dull pain?
The best treatments manage how receptors transmit sharp vs. dull pain by matching the therapy to the dominant pathway rather than treating all pain as if it were the same.
Effective pathway-specific pain management shifts the focus from generic relief to targeting the exact mechanism driving the discomfort. You do not treat a fast superficial sting with the same logic used to treat a deep, dull throb.
How do local anesthetics help when receptors transmit sharp vs. dull pain?
Local anesthetics help when receptors transmit sharp vs. dull pain by blocking voltage-gated sodium channels, which reduces local nerve conduction and is especially useful when sharp, immediate, localized pain is dominant.
Lidocaine physically plugs the sodium channels on the nerve membrane, preventing the nerve from generating the electrical spark needed to send the pain signal. This localized sodium-channel blockade is highly effective for sharp localized pain because it temporarily silences the fast-firing A-delta fibers at the source.
Local and topical anesthetics are established noninvasive or minimally invasive analgesic tools for superficial pain contexts.
How do anti-inflammatories and topical agents help when receptors transmit sharp vs. dull pain?
Anti-inflammatories and selected topical agents help when receptors transmit sharp vs. dull pain by targeting the tissue processes that sustain slower, lingering inflammatory pain after the first sharp signal has passed.
Dull, lingering pain is often driven by inflammatory mediators irritating the unmyelinated C-fibers inside the damaged tissue. Anti-inflammatory support reduces this chemical soup, calming the environment that continuously provokes the slow pain pathway. Minimizing this prolonged inflammation is also a critical factor in how dermal nerves regenerate after injury, as a stable tissue environment prevents damaged free nerve endings from misfiring during the repair phase.
The literature supports NSAIDs as first-line agents for many inflammatory pain states, while topical anesthetic reviews support superficial-procedure and dermal-laceration contexts.
Pathway-Matched Pain Control
- Problem → sharp pain dominates → fast local nerve signaling is the main issue.
- Implication → immediate localized warning is the main clinical target.
- Solution → local numbing strategies may fit best.
- Problem → dull pain dominates → slower ongoing inflammatory or lingering signaling is active.
- Implication → the pain is less about the first warning and more about persistent tissue alarm.
- Solution → anti-inflammatory or longer-acting pain-calming strategies may fit better.
What are the key summary facts for how receptors transmit sharp vs. dull pain?
The key summary facts are that receptors transmit sharp vs. dull pain through A-delta fibers and C-fibers, myelination makes sharp pain arrive first, and pain management works best when it matches the dominant signal type.
Summary Checklist
What steps can you take to treat injuries as receptors transmit sharp vs. dull pain?
Injuries are treated more effectively when receptors transmit sharp vs. dull pain in a recognizable pattern and treatment is matched to whether the dominant signal is immediate and localized or slower and lingering.
Final Execution Checklist
Quick Answers About How Receptors Transmit Sharp vs. Dull Pain
What receptors transmit sharp versus dull pain?
Nociceptors, which are specialized free nerve endings, transmit both sensations. Receptors transmit sharp vs. dull pain by routing the signals through two entirely different biological cables: fast A-delta fibers and slow C-fibers.
Why does sharp pain arrive before dull pain?
Sharp pain arrives first because it travels on myelinated A-delta fibers, which conduct electrical signals at high speeds. Dull pain arrives later because it travels on unmyelinated C-fibers, which conduct signals much more slowly.
What is the difference between A-delta fibers and C-fibers?
A-delta fibers are myelinated and quickly carry sharp localized pain signals to warn you of immediate danger. C-fibers are unmyelinated and carry slow, dull burning aching pain signals to enforce rest and protection.
What is first pain and second pain?
First pain and second pain describe the dual-stage pain response to a single injury. First pain is the initial sharp sting mediated by A-delta fibers, while second pain is the lingering, dull ache mediated by C-fibers.
Do local anesthetics help sharp pain more than dull pain?
Yes. Local anesthetics target fast nerve conduction through sodium-channel blockade, making them highly effective for the immediate, sharp localized pain signal generated during superficial injuries or minor procedures.
Why does dull pain linger longer after injury?
Dull pain lingers longer because C-fibers respond continuously to the inflammatory chemicals released by damaged tissue, creating a sustained, aching pain signal designed to protect the area while it heals.
When do anti-inflammatories fit the pain pattern best?
Anti-inflammatory support fits best when dealing with second pain. By reducing the chemical irritation in the tissue, these medications calm the environment that sustains the slow, dull, aching pain signal.
Conclusion
In conclusion, receptors transmit sharp vs. dull pain through two different systems because the body needs both an immediate warning signal and a slower reminder to protect injured tissue after the first reaction.
By distinguishing between the fast, myelinated A-delta fibers that trigger instant withdrawal and the slow, unmyelinated C-fibers that enforce rest, the two-stage nature of pain becomes biologically clear. Pathway-specific pain management is ultimately more effective than treating all discomfort identically, allowing us to safely quiet the specific alarm that is ringing.