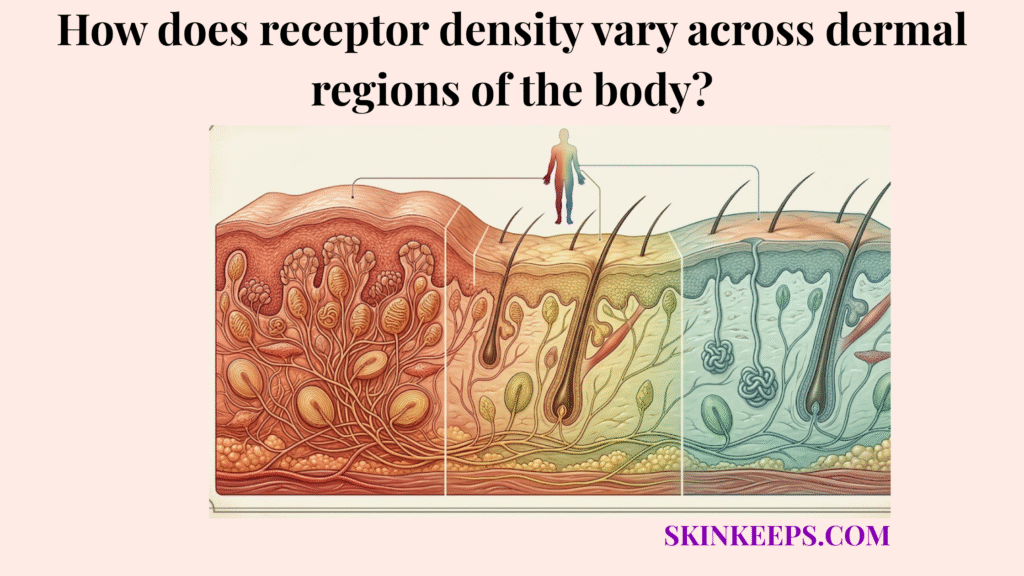
Receptor density varies across dermal regions because the body does not need the same level of tactile precision everywhere, so areas such as the fingertips, lips, and tongue receive denser sensory input than broader lower-resolution regions such as the back and thighs.
The skin operates as a highly specialized sensory map, rather than a uniform or flat sensory sheet. It deliberately concentrates neurocutaneous hardware precisely where environmental interaction is greatest, leaving sweeping tracts of tissue equipped only for baseline defense.
Understanding regional receptor density maps out the tactile baseline first, proves the mechanical truth of two-point discrimination, illustrates how brain processing aligns via the sensory homunculus, compares diverse body zones, and ultimately clarifies why sensory blunting causes debilitating functional loss.
What is the biological baseline for how receptor density varies across dermal regions?
The biological baseline for how receptor density varies across dermal regions is tactile resolution—the ability of a skin region to separate and identify fine touch detail—meaning the more sensory units packed into a region, the more precisely that region can separate, locate, and interpret fine touch.
High-density regions collect massive amounts of independent mechanical data. Because their receptors are tightly clustered, these areas easily separate minute surface differences that sparser regions merge into a single blur.
The two-point discrimination threshold—the ability to perceive two nearby points as separate rather than as one—functions as the definitive proof concept for this capability. Denser regions achieve smaller separation thresholds.
A 2022 Frontiers review reports that human adult skin contains around 200,000–270,000 mechanoreceptor-linked neural fibres, and that the glabrous skin of the young adult hand alone contains about 17,000. The same review also states that the finger pad contains about 100 SA1 units/cm² and 150 RA1 units/cm², with average center-to-center spacing of 1.0 mm and 0.82 mm, respectively. Those values make the basic rule clear: dense receptor packing supports finer tactile resolution (Deflorio, Di Luca, and Wing, 2022).
How does the sensory homunculus explain why receptor density varies across dermal regions?
The sensory homunculus—the cortical body map showing that some body parts receive much larger sensory representation than others—explains why receptor density varies across dermal regions by showing that body parts with denser sensory input receive larger cortical representation and greater perceptual priority.
Because the hands and lips bombard the central nervous system with an immense volume of dense tactile data, the somatosensory cortex dedicates vastly more processing space to decipher those specific signals.
This biological relationship defines cortical magnification—disproportionate brain processing devoted to a small but sensory-important body region. Peripheral density explicitly dictates brain allocation.
StatPearls describes the sensory homunculus as a topographic map of bodily sensation in cortex and notes that the face occupies the most area, while the hand is also strongly represented in the lateral sensory cortex (Nguyen and Duong, 2023) (Raju and Tadi, 2022).
How does functional necessity dictate how receptor density varies across dermal regions?
Functional necessity dictates how receptor density varies across dermal regions because the body concentrates sensory detail where precise tactile feedback is most important for control, interaction, and protection.
The fingertips require massive sensory input to manipulate tools, regulate grip force, and identify structural faults. Fine motor control demands uncompromised tactile acuity, the sharpness and precision of the touch signal.
The lips and face navigate temperature, food texture, and intimate contact, demanding equally fine data. In direct contrast, broader sections of the body operate simply to report blunt trauma or general pressure, requiring drastically fewer sensors to achieve their protective mission.
How do sensitive and insensitive zones compare in how receptor density varies across dermal regions?
Sensitive and insensitive zones differ because receptor density varies across dermal regions according to tactile demand, with high-detail areas receiving denser sensory packing than broad lower-resolution regions.
High-density sensory zones prioritize discrimination and measurement. Low-density sensory zones prioritize broad coverage and efficiency over granular detail.
Comparing these extremes proves the regional density principle. NCBI Clinical Methods reports classic two-point discrimination values of 1 mm at the tongue tip, 2–4 mm at the fingertip, 8–12 mm at the palm, and 20–30 mm at the dorsum of the hand. These values show that tactile resolution differs sharply by body region and support comparison between dense and less-dense sensory zones (Bigley, 1990).
| Body region | Relative receptor density | Typical tactile resolution pattern | Main functional purpose |
|---|---|---|---|
| Fingertips | Very high | ~2–4 mm two-point range | Fine grip, texture, object control |
| Lips / tongue | Very high | Very high; tongue tip ~1 mm | Feeding, speech-related contact, fine sensory awareness |
| Palms | Moderate | ~8–12 mm two-point range | Contact awareness and manual interaction |
| Back / thighs / upper arms | Low | Lower than high-density zones | Broad contact and protective awareness |
How do high-density dermal regions improve tactile resolution when receptor density varies across dermal regions?
High-density dermal regions improve tactile resolution because more sensory units collect more detailed mechanical information from the same area of skin.
A smaller receptive field—the area of skin from which a sensory unit receives input—ensures that mechanical forces do not blur together. This sharpens the two-point separation capability immediately.
The density radically enhances texture discrimination and slip detection. By monitoring micro-vibrations across tightly grouped units, the skin precisely regulates object control and grip.
The same 2022 Frontiers review reports that the finger pad contains about 100 SA1 units/cm² and 150 RA1 units/cm², with receptive-field spacing of approximately 1.0 mm and 0.82 mm. It also notes that the hand carries a much higher concentration of tactile afferents than many larger body regions. These values give the clearest quantitative explanation for why dense tactile zones perform better (Deflorio, Di Luca, and Wing, 2022).
How do low-density dermal regions function when receptor density varies across dermal regions?
Low-density dermal regions still function effectively because they are designed for broader, lower-resolution sensation rather than for fine tactile discrimination.
Sparse distributions do not equal useless sensation; they simply gather a different caliber of data. They detect broad touch, generalized pressure, and threat vectors adequately. The nervous system avoids wasteful allocation by dropping precision on the back. This preserves central processing power while maintaining full-body protective awareness.
What clinical factors alter how receptor density varies across dermal regions?
Clinical factors alter how receptor density varies across dermal regions by reducing the effective sensory resolution of regions that normally depend on dense tactile input.
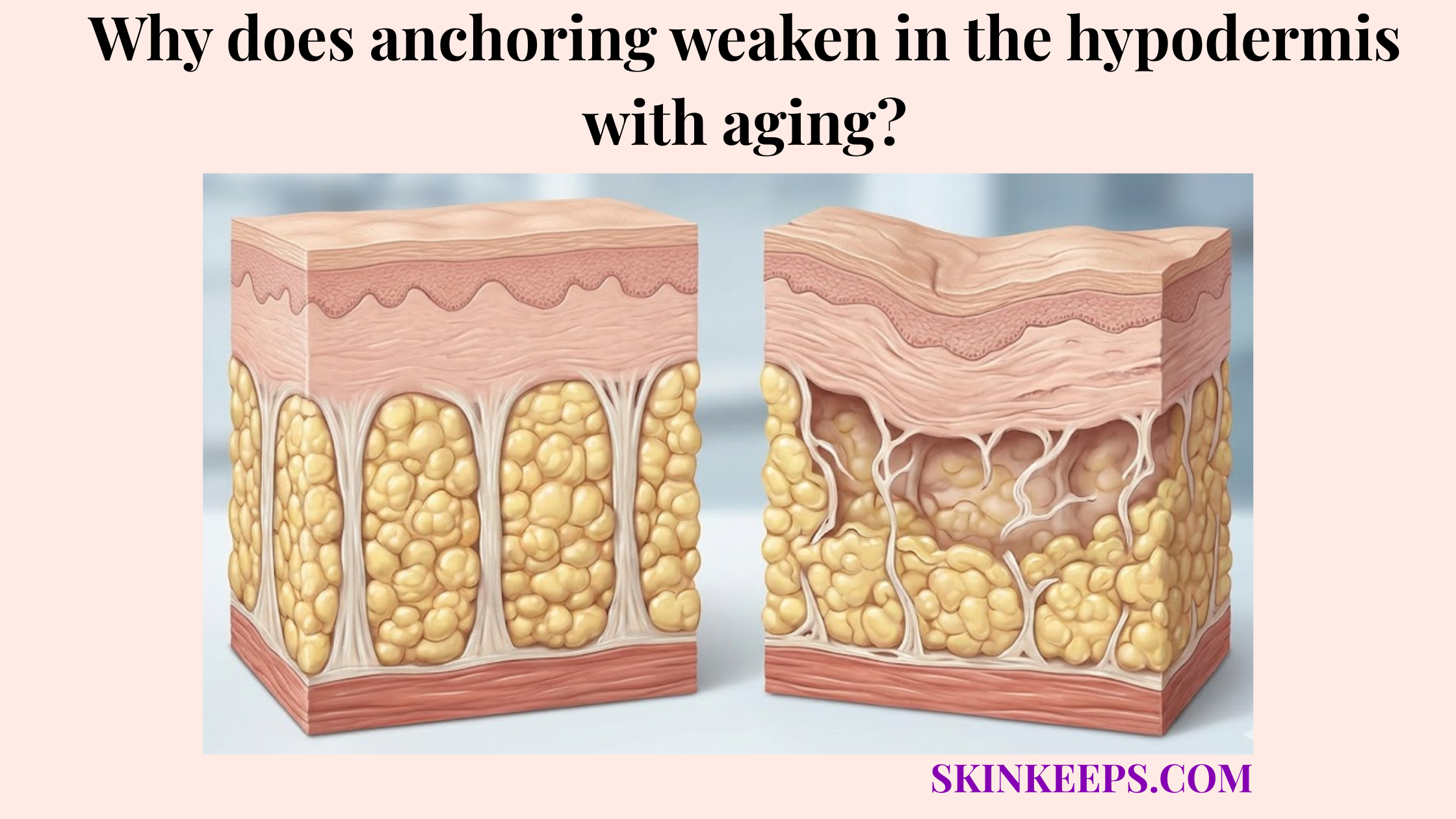
Sensory maps face deterioration over time. Aging inherently diminishes structural vitality, while metabolic diseases induce toxic degradation.
This blunting forces previously high-resolution areas to function like low-resolution zones, dangerously impairing fine motor control and safety.
How does aging alter how receptor density varies across dermal regions?
Aging alters how receptor density varies across dermal regions by reducing the effectiveness and, in some receptor classes, the density of tactile sensory units in regions that depend on high-resolution fine touch.
Age-related tactile decline blunts precision, specifically handicapping the dense zones that navigate detail. This reduction slowly degrades environmental feedback clarity and fine dexterity.
The 2022 Frontiers review cites evidence that the number of Meissner and Merkel receptors in the 60–90 year age group can be four to six times lower than in adults aged 20–49 years. These figures support age-related blunting of effective tactile precision in dense sensory zones (Deflorio, Di Luca, and Wing, 2022).
How does peripheral neuropathy alter how receptor density varies across dermal regions?
Peripheral neuropathy alters how receptor density varies across dermal regions by damaging sensory endings and nerve pathways, especially in high-value tactile zones such as the hands and feet.
Neuropathic damage actively hollows out the functional map, inducing aggressive sensory blunting—the reduced sharpness or clarity of touch perception. This creates functional sensory dead zones where dense receptors previously thrived.
A 2021 Journal of Clinical Medicine study reported that Meissner corpuscle density was reduced by about 80% in non-painful diabetic distal symmetric polyneuropathy and was almost completely absent in the painful form. The same study also found a 68% reduction in Merkel-cell density in the non-painful group and a 93% reduction in the painful group. These figures justify describing neuropathy as a process that can create functional sensory dead zones in normally dense tactile regions (García-Mesa et al., 2021).
Sensory Decline Pathway
- Problem → Receptor performance or nerve support declines.
- Implication → Tactile resolution becomes blurred in high-density regions.
- Solution → Protect nerve health, manage metabolic stress, and monitor sensory change.
What are the key summary facts for how receptor density varies across dermal regions?
The key summary facts are that receptor density varies across dermal regions according to tactile demand, high-density regions deliver better fine-touch resolution, and clinical decline can reduce the effective precision of those regions over time.
Dermal Density Summary Checklist
What steps can you take to protect your sensitivity as receptor density varies across dermal regions?
Sensitivity is best protected when high-value tactile regions and the nerve pathways that serve them remain structurally and metabolically healthy.
Sensory Preservation Execution Checklist
Quick Answers About How Receptor Density Varies Across Dermal Regions
Why is receptor density higher in fingertips than in the back?
Receptor density varies across dermal regions because fingertips demand fine tactile discrimination for grasping and object interaction, while the back requires only broad protective awareness. The body allocates dense sensory input where fine motor control is functionally required.
Which dermal regions have the highest tactile receptor density?
The fingertips, lips, and tongue exhibit the highest tactile receptor density. These high-density sensory zones process intricate mechanical textures, enabling precise sensory interactions that broader skin regions cannot match.
What does two-point discrimination reveal about receptor density?
The two-point discrimination threshold reveals exactly how receptor density varies across dermal regions. A 2–4 mm threshold at the fingertip confirms dense receptor packing, while a 20–30 mm threshold on the hand’s dorsum confirms a sparse, low-density distribution. (Bigley, 1990)
Why do lips and tongue have high tactile resolution?
Lips and the tongue possess exceptionally high tactile resolution to govern delicate feeding, speech articulation, and facial contact. Dense sensory input in these regions guarantees immediate, highly localized responses to structural textures and shapes.
How does the sensory homunculus relate to receptor density?
Sensory homunculus mapping visually reflects how receptor density varies across dermal regions. Because the fingertips and lips send massive amounts of tactile data, the somatosensory cortex allocates disproportionate cortical magnification to process those specific regions.
Can neuropathy blunt high-density tactile regions?
Yes. Neuropathic sensory blunting destroys nerve pathways, turning historically dense areas into functional sensory dead zones. In severe diabetic neuropathy, Meissner corpuscle density drops by over 80%, obliterating fine tactile discrimination. (García-Mesa et al., 2021)
Does aging reduce fine tactile discrimination?
Yes, age-related tactile decline significantly reduces fine tactile discrimination. In adults aged 60–90, tactile sensory units like Meissner and Merkel receptors can be four to six times lower than in younger demographics, diminishing tactile acuity. (Deflorio, Di Luca, and Wing, 2022)
Conclusion
In conclusion, receptor density varies across dermal regions because tactile precision is distributed according to functional need, with dense sensory zones supporting fine discrimination and lower-density zones supporting broader protective awareness.
By mapping dense tactile input from the fingertips directly to magnified cortical representation, the body achieves perfect sensorimotor control where it matters most. While peripheral neuropathy and age-related decline inevitably blunt this sharpness over time, the underlying blueprint proves that human skin acts as a remarkably intelligent, regionally specialized defensive and sensory organ.