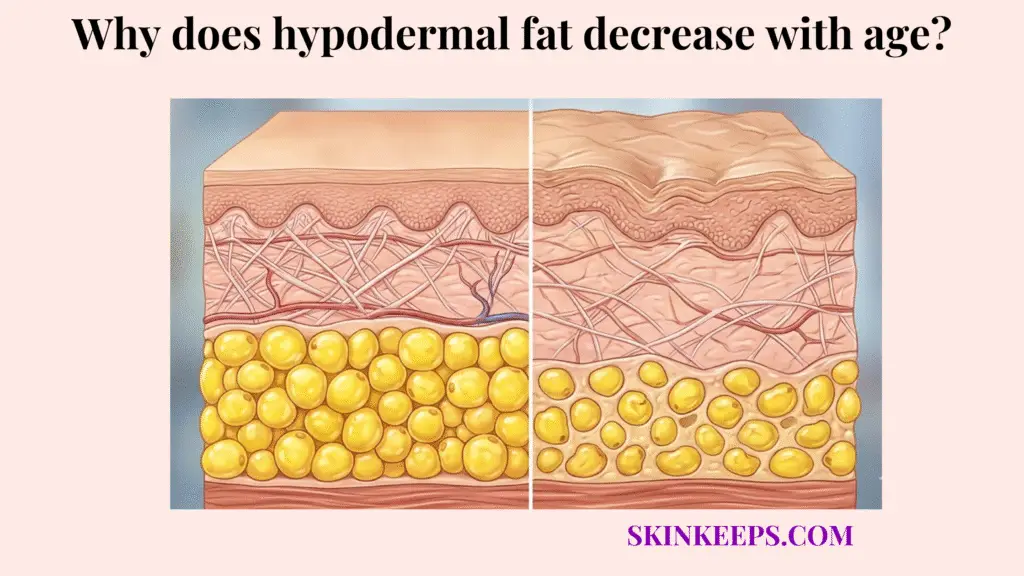
Hypodermal fat decreases with age because the subcutaneous tissue gradually loses adipocyte renewal strength, metabolic resilience, structural support, and region-specific volume stability over time. This foundational layer, residing beneath the dermis, dictates the youthful contour and mechanical cushioning of the face and body. The biologic progression is a distinct aging phenomenon, reflecting an intrinsic breakdown rather than simply an energy-storage deficit.
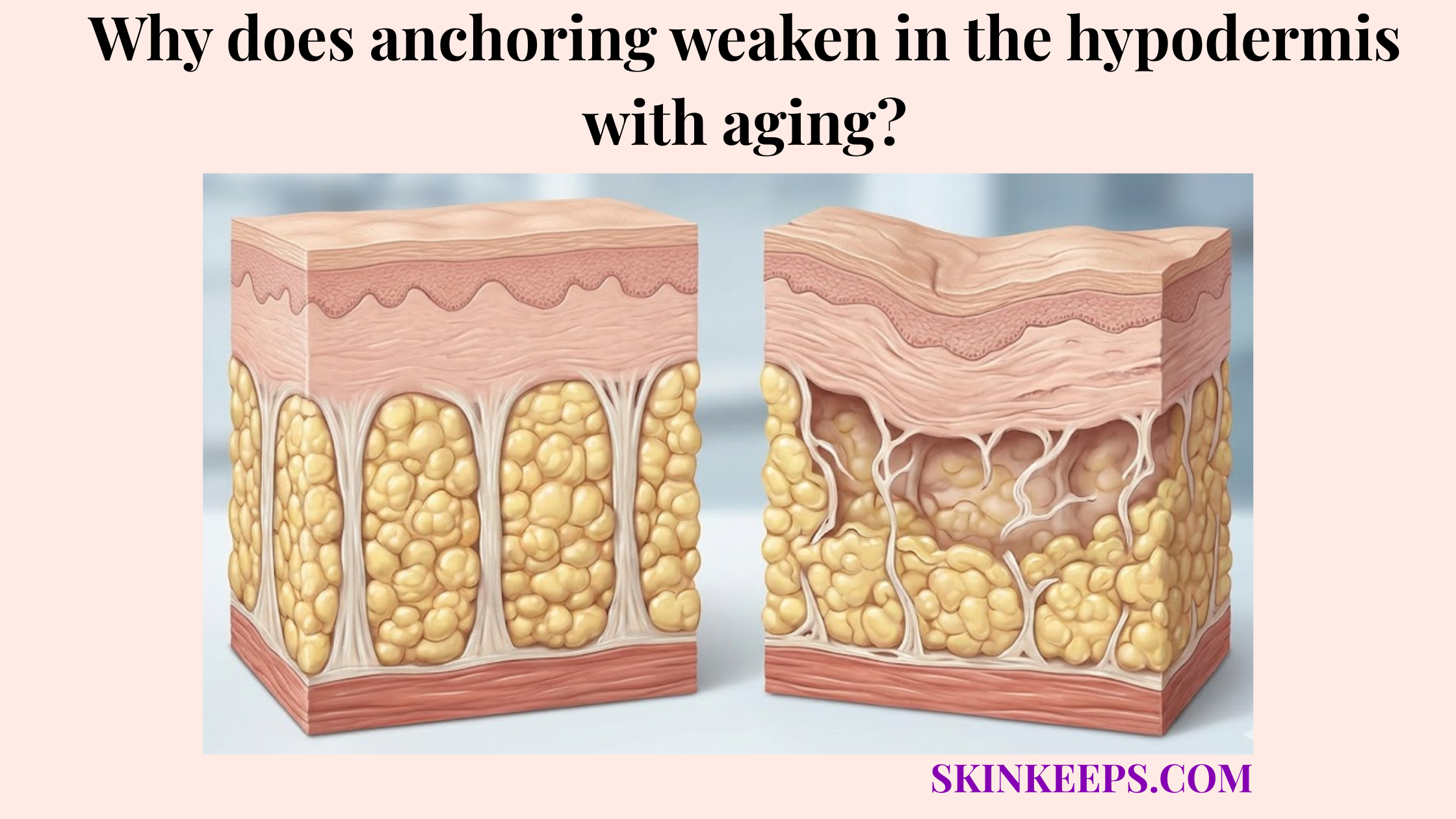
The decline reflects both profound fat-cell aging and widespread deep structural support degradation. It is not a straightforward emptying of lipid reserves; instead, the cells that manage fat storage become less efficient, and the fibrous matrix that holds them in optimal architectural positions weakens. Consequently, the tissue loses its innate ability to fight against gravity and mechanical stress, leading to a permanent structural shift.
To fully grasp this physiologic evolution, it is necessary to examine the mechanisms in sequence. This clinical article will navigate the definition of deep-tissue thinning, the cellular causes behind it, its stark differences from ordinary weight loss, and the regional patterns where it manifests most visibly. Furthermore, we will explore the chronological timeline of this decline, the most biologically appropriate treatments for restoration, the lifestyle habits that accelerate the aging process, the common clinical mistakes to avoid, and a final biologic recap of age-related soft-tissue depletion.
What Exactly Is Age-Related Hypodermal Fat Loss?
Age-related hypodermal fat loss is the gradual thinning, weakening, and structural decline of the deep subcutaneous layer that normally provides padding, energy storage, insulation, and soft-tissue support. The hypodermis acts as the innermost architectural tier of the integumentary system, constructed of organized lobules of adipocytes encased in a robust fibrous septal network. When observing the clinical disparities between young and mature tissue profiles, the majority of the structural volume deficit originates directly within this deep compartment rather than the superficial layers.
When this specific tissue layer thins naturally over the lifespan, the physical and physiological consequences extend far beyond mere visual deflation. The biologic structure loses its protective padding capability, resulting in diminished mechanical shock absorption and a pronounced topographical prominence of underlying skeletal and muscular frameworks. Visually, this intrinsic failure translates into progressive surface hollowing, structural laxity, and contour collapse that superficial dermatological interventions cannot adequately resolve.
This complex deep-volume decline reflects an interconnected trajectory of cellular senescence and extracellular matrix deterioration occurring simultaneously. It represents a state where the resident adipocytes lose metabolic vitality while their surrounding structural scaffolding gradually disintegrates. There is no universally accepted single percentage for whole-body age-related hypodermal thinning, as the process remains highly localized and anatomically variable across distinct physiological zones, demanding targeted clinical understanding (Liu et al., 2024) [PMC].
What Cellular and Biochemical Changes Cause Age-Related Hypodermal Fat Loss?
Cellular and biochemical changes cause age-related hypodermal fat loss by reducing adipocyte renewal, altering adipose-cell function, and weakening the biologic environment needed to preserve healthy subcutaneous volume. As mammalian tissue matures, it suffers from a dramatically diminished pool of viable mesenchymal stem cells, sharply limiting its capacity to orchestrate robust adipogenesis. Because fewer new fat cells are created to replace dying ones, this natural thinning of the hypodermis is fundamentally a regenerative-failure problem.
The core physiological foundation of this persistent decline is rooted in both reduced adipogenesis and the onset of profound fat-cell aging and dysfunction. Older adipocytes inherently exhibit altered metabolic signaling, often secreting inflammatory cytokines while gradually losing their optimal lipid-storing architecture—a degradative state scientifically recognized as cellular senescence. This paracrine aging effect creates a biochemically hostile microenvironment that actively accelerates the enzymatic destruction of the surrounding collagenous septae, unmooring the fat lobules from their structural anchors.
Adding a critical hormonal context to this biologic shift, the menopause-linked decline in estrogen profoundly accelerates changing adipose maintenance and its anatomical distribution. Estrogen normally exerts a vital protective, proliferative effect on subcutaneous connective tissues, and its systemic withdrawal irrevocably destabilizes deep fat compartments. To illustrate this acceleration mathematically, a menopause-focused skin review notes that up to 30% of skin collagen may be lost in the first 5 years after menopause, highlighting how sharply structural aging can accelerate during periods of severe estrogen decline (Thornton, 2013) [PMC].
| Aging-related change | Biological mechanism | Effect on fat cells |
|---|---|---|
| Reduced renewal | Lower adipogenesis and differentiation | Fewer newly functional adipocytes |
| Altered adipocyte function | Metabolic and paracrine aging | Lower tissue resilience |
| Structural support decline | Weaker connective scaffolding | Less stable fat-pad behavior |
| Hormonal shift | Menopause/estrogen-related redistribution | More visible midlife volume change |
| Combined tissue aging | Cellular + matrix decline together | Progressive deep volume loss |
How Does Subcutaneous Fat Depletion From Aging Differ From Ordinary Weight Loss?
Subcutaneous fat depletion from aging differs from ordinary weight loss because aging changes the biologic quality, regenerative capacity, and structural support of the tissue, while ordinary weight loss mainly changes body fat amount and adipocyte size. This fundamental distinction is one of the most critical concepts in clinical dermatology. When a patient diets, the cells simply release stored lipids; when a patient ages, the underlying tissue scaffold actively deteriorates and the cellular population loses its physiological fitness.
Losing an identical amount of numerical weight at age 25 versus age 50 yields entirely different visual outcomes precisely because the tissue scaffold is not equally robust. In younger tissue, the tight septal network acts like an elastic corset, instantly rebounding and keeping the remaining fat lobules optimally positioned. In mature, structurally compromised tissue, weight loss exacerbates the preexisting biologic laxity, creating stark deflation, descending tissues, and a highly skeletal appearance rather than a smoothly contoured silhouette.
Furthermore, the clinical reversibility of these two processes varies drastically. Ordinary caloric-deficit weight loss can often be partially or fully regained through targeted nutrition and body-mass restoration. Conversely, aging-related decline is significantly harder to reverse autonomously because the biologic environment has permanently shifted. Highlighting this persistent depth of change, a quantitative midface aging study found that over an average of 11.3 years, subjects permanently lost 11.3% of superficial fat volume and 18.4% of deep fat volume in the midface, confirming profound biologic depletion rather than transient weight fluctuation (Boehm et al., 2021) [PubMed].
| Feature | Age-related fat loss | Ordinary weight loss |
|---|---|---|
| Main biological difference | Tissue aging | Energy deficit |
| Main driver | Biology vs body-mass change | Body-mass reduction |
| Structural support | Aging changes support | Often better preserved |
| Reversibility | Limited by tissue decline | Often more reversible |
| Visible effect | Hollowing + descent + laxity | Deflation with less structural failure |
| Best response | Protection + structural treatment | Nutrition / weight restoration |
Which Body Regions Show Facial and Structural Volume Loss Most Visibly as We Age?
Facial and structural volume loss becomes most visible in regions where subcutaneous support is thin, mobile, repeatedly exposed, or functionally important, especially the face, hands, and pressure-bearing areas. Because age-related hypodermal decline operates distinctly across different physiological zones, the body does not atrophy uniformly. Clinicians must map this specific depletion to understand why certain topographical features abruptly transform during the aging trajectory.
Cosmetically, the face is the most profoundly visible canvas for this progression. The highly compartmentalized fat pads of the cheeks, under-eyes, and temples systematically thin and descend, resulting in pronounced shadowing and a skeletal contour. Following the facial decline, the dorsal surface of the hands exhibits dramatic aging; as the minimal subcutaneous cushioning depletes, the underlying network of veins, tendons, and bony joints becomes starkly unmasked. Subsequently, pressure-bearing regions, such as the plantar fat pads of the feet, experience profound mechanical wear and volumetric loss.
It is vital to recognize that while some regions are scrutinized mainly for aesthetic appearance, other regions suffer deep functional and physical comfort consequences. Losing midface volume alters cosmetic identity, but losing plantar cushioning severely diminishes shock absorption and walking comfort. As previously noted, the strongest quantitative evidence for this regional specificity lies in the face, where studies tracked an 18.4% deep fat-volume loss over roughly a decade, establishing the precise, measurable reality of this compartment-specific depletion (Boehm et al., 2021) [PubMed].
| Body Region | Typical Pattern of Decline | Functional / Visible Effect |
|---|---|---|
| Midface / cheeks | Compartment thinning and descent | Hollowing, flattening, sharper contours |
| Temples / under-eyes | Local volume loss | Shadowing, skeletal appearance, “tired” look |
| Hands | Dorsal thinning | Visible veins, tendons, joints |
| Soles / plantar pads | Cushioning loss | Mechanical discomfort, reduced shock absorption |
At What Chronological Age Does the Natural Thinning of the Hypodermis Become Clinically Noticeable?
The natural thinning of the hypodermis becomes clinically noticeable gradually rather than at one exact age, with silent biologic changes often beginning earlier and more visible structural volume loss becoming easier to recognize across the 40s, 50s, and later decades. Patients frequently seek an absolute chronological threshold, but soft-tissue depletion operates as an insidious continuum. The biological mechanisms—such as the slowing of cellular regeneration and subtle collagen fibril fragmentation—quietly initiate beneath the surface long before the mirror reflects a tangible deficit.
In clinical practice, a clear decade-based progression is routinely observed. During the 30s, subclinical volumetric slowdowns commence, largely masked by lingering tissue elasticity. As individuals progress through their 40s and 50s, the synergistic decline of bone density, ligament strength, and adipocyte volume triggers a precipitous architectural collapse, making the structural shifts undeniably visible. By the 60s and beyond, the profound depletion of deep support layers dictates advanced contour hollowing and definitive mechanical laxity.
Furthermore, it is critical to underscore that individual biological timelines are aggressively modulated by external lifestyle and internal systemic factors. Genetics, severe ultraviolet exposure, smoking habits, and chronic weight cycling can prematurely propel the tissue into an aged state. Anchoring this chronology physiologically, the aforementioned 11.3-year facial tracking study alongside the severe menopause-related structural acceleration data confirms that while exact timing fluctuates, clinically relevant midface depletion is intensely progressive and universally unmasked by midlife (Boehm et al., 2021; Thornton, 2013) [PubMed].
Which Clinical Treatments Best Restore Age-Related Loss of Fat Under the Skin?
The clinical treatments that best restore age-related loss of fat under the skin are those that either replace lost volume directly or rebuild structural support around it, especially biostimulating fillers, selected hyaluronic acid fillers, and autologous fat grafting. Recognizing that surface topicals cannot reach the hypodermis is paramount. The appropriate intervention must respect the depth of the anatomical void, matching the volumetric tool precisely to the missing biological structure.
Clinicians analyze treatments based on distinct versions of the same core problem. Hyaluronic acid (HA) fillers are expertly formulated to manage immediate focal hollowness, providing targeted projection to highly localized skeletal deficits. Conversely, biostimulating agents like Poly-L-lactic acid (PLLA) or Calcium hydroxylapatite (CaHA) act functionally to instigate neocollagenesis, rebuilding the diffuse connective-tissue structural support rather than merely inflating the space artificially.
The ultimate treatment choice demands a nuanced assessment of the patient’s existing tissue quality, extent of loss, acceptable downtime, and financial parameters. For massive, broad-spectrum volume replacement, autologous fat grafting remains a powerful deep-tissue intervention. It is imperative to note, however, that clinical literature reports high volume-retention variability in fat grafting, frequently clustering around typical retention rates of roughly 40% to 68% depending on technique and physiological acceptance, showcasing that while robust, it is not flawlessly predictable (Groen et al., 2017; Schipper et al., 2022) [PMC].
| Treatment Type | Cost | Downtime | Best For Aging Tissue |
|---|---|---|---|
| Hyaluronic acid filler | Lower to moderate | Low | Immediate focal hollows |
| Biostimulator filler (PLLA / CaHA) | Moderate | Low to moderate | Diffuse structural support |
| Autologous fat grafting | Higher | Higher | Larger or broader deep-volume restoration |
Which Daily Habits Should You Avoid to Prevent Accelerated Age-Related Facial Volume Loss?
To prevent accelerated age-related facial volume loss, you should avoid the daily habits that add structural damage or destabilize soft-tissue volume, especially heavy UV exposure, smoking, and repeated weight cycling. While intrinsic chronological aging is biologically programmed, extrinsic lifestyle accelerators radically magnify the severity and early onset of soft-tissue failure. These habits aggressively dismantle the remaining connective architecture that prevents adipose tissue from rapidly descending.
The biological rationale for avoiding UV radiation and smoking extends far past superficial wrinkle prevention. Heavy ultraviolet exposure generates matrix metalloproteinases (MMPs), destructive enzymes that literally shear apart the deeper collagenous bands suspending the hypodermal fat. Similarly, the systemic vasoconstriction and toxic oxidative stress induced by smoking aggressively starve the adipocytes and connective tissues of vital oxygen, permanently weakening the regenerative viability of the deep compartment.
Equally critical is the practical avoidance of chronic weight cycling—a highly destructive mechanical accelerator often dismissed in cosmetic discussions. Rapidly oscillating body mass repeatedly hyper-expands and abruptly deflates the septal corset of the hypodermis, eventually destroying its elastic recoil. As a foundational prevention tool, consistent broad-spectrum protection is vital, considering that SPF 30 sunscreen effectively filters approximately 97% of UVB rays, mitigating immense photoaging pressure from the deeper underlying scaffolding (NCBI Bookshelf, 2018) [PMC].
What Are the Most Common Treatment Mistakes to Avoid When Addressing Natural Thinning of the Hypodermis?
The most common treatment mistakes to avoid when addressing natural thinning of the hypodermis are using surface-level solutions for deep structural loss, overusing energy-based devices, and adding volume without respecting the tissue’s weakened support. A profound biological error occurs when practitioners or patients attempt to resolve an anatomical volume void with treatments designed strictly for superficial textural refinement. Proper aesthetic restoration requires a precise matching of the therapy to the exact physiological depth of the deterioration.
Because aging tissue possesses an inherently fragile structural matrix, what constitutes a “good treatment” dynamically shifts as the patient matures. Vigorously injecting massive quantities of dense filler into a heavily weakened retaining ligament network will inevitably result in unnatural distortion and accelerated tissue drooping. Mature tissue simply cannot support heavy volumetric loads in the exact manner that youthful, collagen-rich tissue can.
Furthermore, an aggressive misuse of deep-penetrating technologies serves as a severe clinical pitfall. Overusing highly calibrated thermal tools in an effort to “tighten” skin can inadvertently liquidate the precious remaining fat reserves. Underscoring this immense risk, a recent major safety anchor is the FDA’s 2025 communication explicitly warning that certain radiofrequency (RF) microneedling complications can include permanent fat loss, alongside burns and disfigurement, heavily supporting caution against aggressive energy use in hollowed terrain (FDA Safety Communication, 2025) [PMC].
What Are the Core Biological Facts to Remember About Age-Related Fat Pad Depletion?
The core biological facts to remember are that age-related fat pad depletion is a cellular and structural aging process, not merely a calorie-loss event, and that it is driven by reduced adipocyte renewal, altered tissue behavior, and weakened support over time. This foundational reality governs all successful aesthetic interventions. Clinicians and educated patients must recognize that this form of soft-tissue failure is an intricate deep-volume aging disease, completely segregated from the transient fluctuations associated with diet and physical conditioning.
The three predominant pillars sustaining this decline are the catastrophic failure of adipogenesis, the irreversible enzymatic shredding of the connective-tissue scaffolding, and the highly predictable regional topographical shifts. By understanding that senescent fat cells actively poison their surrounding structural environment, it becomes radically clear why simply attempting to “gain weight” fails to restore a youthful, lifted contour to a structurally collapsed midface.
Ultimately, long-term volumetric preservation and restoration must directly interface with the structural depth of the crisis. Addressing this effectively demands therapies engineered to rebuild deep architecture rather than masking the surface. Keeping these realities anchored, clinical evidence like the 18.4% deep midface fat loss measured over 11.3 years, paired with the massive postmenopausal collagen failure, serve as the ultimate reminders of how rapidly structural aging permanently reshapes our anatomy (Boehm et al., 2021; Thornton, 2013) [PubMed].
Biological Recap Checklist
Quick Answers About Age-Related Hypodermal Fat Loss
Is hypodermal fat loss the same as losing weight?
No. Hypodermal fat loss from aging involves the biological deterioration of adipocyte function and the breakdown of structural connective tissue, whereas ordinary weight loss primarily involves the shrinkage of fat cells due to an energy deficit without the complete collapse of the biological scaffold.
Why does facial volume loss look worse with age?
Facial volume loss looks worse with age because the deep support layer thins simultaneously with the weakening of retaining ligaments and the loss of skin elasticity. This compounding structural failure causes fat pads to deflate and descend, leading to visible hollowing, shadowing, and skeletal prominence.
Can skincare rebuild deep fat loss?
Skincare cannot rebuild deep fat loss. Topical products penetrate only the epidermis and occasionally the upper dermis. They are biologically incapable of reaching the deep hypodermis to stimulate new adipogenesis or restore structurally depleted subcutaneous volume.
Does menopause make volume loss worse?
Yes, menopause significantly accelerates volume loss. The sudden drop in systemic estrogen weakens the collagenous scaffolding that supports deep fat compartments, leading to rapid structural instability, altered fat distribution, and more pronounced facial hollowing.
What is better for larger volume loss: filler or fat grafting?
Autologous fat grafting is generally better for larger, diffuse structural volume loss because it replaces living tissue and provides broader systemic support. Hyaluronic acid fillers are typically better suited for immediate, localized focal hollowing.
Are RF devices always safe for hollow faces?
No. Aggressive use of radiofrequency (RF) energy devices in already hollow or fat-depleted faces can be risky. If the thermal energy penetrates deeply into an already weakened hypodermis, it can inadvertently damage remaining viable adipocytes and worsen the skeletal appearance.
Why do hands show age-related volume loss so clearly?
Hands show age-related volume loss clearly because the dorsal (back) surface of the hand naturally possesses very little subcutaneous fat and thin overlying skin. As this minimal cushioning depletes with age, underlying veins, tendons, and bony structures immediately become highly visible.
Can stable weight help preserve facial volume?
Yes, maintaining a stable weight helps preserve facial volume by preventing repeated mechanical stress on the connective tissue matrix. Chronic weight cycling stretches and damages the septal network that holds fat pads in place, accelerating premature sagging and structural laxity.
Conclusion
Hypodermal fat decreases with age because the tissue gradually loses regenerative strength, structural support, and stable compartment behavior, producing a form of deep volume decline that is biologically different from ordinary dieting-related fat change. The hypodermis is essentially the body’s premier biological cushion, and its persistent deterioration profoundly alters both functional mechanics and aesthetic silhouettes.