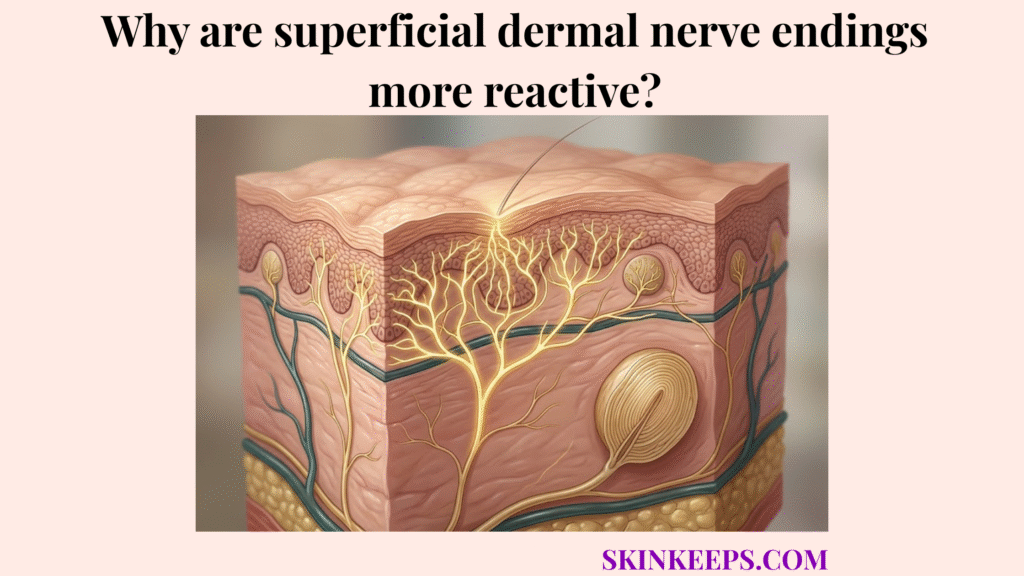
Superficial dermal nerve endings are more reactive because they sit close to the epidermal surface, where even minor injury can expose them to air, movement, temperature change, and chemical irritation.
A paper cut or superficial scrape can sting far more than a deeper bruise or narrow puncture because the shallow damage specifically targets and uncovers these sensitive surface alarm systems, leaving them raw and continuously triggered.
Understanding this reactivity requires examining the baseline anatomy of pain sensors, exploring how exposure amplifies firing, mapping receptor density across the body, comparing surface versus deep injuries, and applying targeted pain-calming treatments.
What is the biological baseline for why superficial dermal nerve endings are more reactive?
The biological baseline for why superficial dermal nerve endings are more reactive is that pain begins in free nerve endings and nociceptors, which are positioned to detect damaging surface stimuli quickly and convert them into neural alarm signals.
Free nerve endings function as unsheathed sensory extensions that penetrate upward into the tissue to detect damaging or potentially damaging stimuli. Nociceptors operate as specialized pain-sensing receptors that capture harmful mechanical, thermal, or chemical input across the skin barrier.
These endings act as the first-line pain sensors located primarily within the papillary dermis, right below the epidermal junction. This specific placement ensures that any breach in the skin instantly activates the neural warning system.
Pain-pathway references identify 2 major nociceptive fiber types: A-delta fibers and C fibers. A-delta fibers mediate the first sharp, fast pain signal, while C fibers mediate the slower burning or aching component. That two-fiber distinction is the clearest quantitative foundation for explaining why superficial injuries can feel both sharply immediate and persistently sore (Kendroud et al., 2022) (Gadhvi and Mendez, 2023).
How does anatomical exposure explain why superficial dermal nerve endings are more reactive?
Anatomical exposure explains why superficial dermal nerve endings are more reactive because a breached epidermal surface leaves injured upper-level pain endings vulnerable to ongoing environmental contact.
An epidermal breach immediately strips away the protective lipid layers and mature cells that normally insulate the dermis. This directly explains how barrier disruption increases tissue vulnerability.
This exposure subjects the superficial pain endings to air, evaporative irritation, touch, water, friction, and surface chemicals, keeping them in a state of repeated restimulation.
Consequently, a small superficial wound continues to hurt long after the initial injury because the environment constantly re-triggers the exposed nerves.
Burn literature provides the strongest natural proof here: superficial partial-thickness burns are described as very painful because nerve endings remain intact and irritated, while deep partial-thickness burns may be less painful because many nerve endings are already damaged. The same source notes healing ranges of 2 to 3 weeks for superficial partial-thickness burns versus longer healing for deeper burns, reinforcing that pain intensity is not linearly proportional to visible depth (Warby and Maani, 2023) (Walker et al., 2023).
How does receptor density explain why superficial dermal nerve endings are more reactive?
Receptor density explains why superficial dermal nerve endings are more reactive because injuries in densely innervated surface regions can activate more nearby pain endings within a very small area.
A densely innervated region concentrates sensory receptors to maximize tactile acuity, meaning any trauma here triggers a massive local alarm.
The fingertips, toes, lips, and facial skin serve as the primary anatomical examples of this extreme sensory concentration. This distribution perfectly maps to how receptor density varies across dermal regions of the body.
This creates a spatial summation effect, where the activation of many tightly packed nociceptors simultaneously amplifies the pain signal transmitted to the brain.
How do surface and deep dermal sensors compare when superficial dermal nerve endings are more reactive?
Surface and deep dermal sensors compare differently because superficial dermal nerve endings react to exposed, fast-changing stimuli more continuously, while deeper sensors are less directly restimulated by the outside environment.
Superficial sharp pain activates instantly to external breaches, while dull deep-tissue pain responds to heavier, crushing forces or internal tissue strain.
The upper dermis prioritizes immediacy and ongoing reactivity to secure the surface, whereas the deep dermis signals broad structural damage without the constant sharp stinging provoked by air exposure.
| Nerve depth | Main trigger pattern | Sensation quality | Reactivity pattern |
|---|---|---|---|
| Superficial dermis | Air, minor trauma, temperature shift, surface irritants | Sharp, stinging, immediate | High ongoing reactivity |
| Deeper tissue | Stronger pressure, deeper deformation, tissue strain | Dull, heavy, less exposed | Lower continuous surface reactivity |
What treatments manage pain when superficial dermal nerve endings are more reactive?
The most useful treatments manage pain when superficial dermal nerve endings are more reactive by insulating exposed tissue, reducing repeated surface stimulation, and dampening local nerve firing when appropriate.
Effectively controlling superficial wound pain requires shifting from a simple healing mindset to a targeted pain-calming treatment logic.
How does sealing exposed skin help when superficial dermal nerve endings are more reactive?
Sealing exposed skin helps when superficial dermal nerve endings are more reactive because occlusive or moist coverage limits air exposure, friction, and direct environmental contact with damaged nerve endings.
Utilizing hydrocolloid dressings, liquid bandages, or a protective ointment safely isolates the raw tissue from environmental triggers.
The main goal is complete insulation, reducing the repetitive restimulation that forces A-delta fibers to fire continuously.
A 2008 hydrocolloid review reported that one acute-wound comparison found 91% pain-free outcomes with the occlusive dressing versus 30% with conventional treatment, alongside a shorter healing time in that study (Thomas, 2008).
How do topical anesthetics help when superficial dermal nerve endings are more reactive?
Topical anesthetics help when superficial dermal nerve endings are more reactive by reducing local pain transmission at the wound surface and making sharp superficial pain easier to tolerate.
Common pharmacological agents like lidocaine and benzocaine act directly on the local nerve endings to halt signal transmission.
This intervention remains limited to superficial pain control, targeting the localized overfiring rather than offering universal deep tissue repair.
Pain Management Pathway
- Problem → superficial nerve endings are exposed and overfiring.
- Implication → sharp pain keeps restarting with air, motion, or contact.
- Solution → insulate the surface, reduce irritation, and blunt local nerve firing when appropriate.
What are the key takeaways and immediate steps when superficial dermal nerve endings are more reactive?
The key takeaway is that superficial dermal nerve endings are more reactive because they are positioned near the surface, are easier to expose after shallow injury, and are easier to restimulate after the original trauma.
Summary Points
Final Execution Checklist
Quick Answers About Why Superficial Dermal Nerve Endings Are More Reactive
Why do tiny shallow cuts sting so much?
Tiny shallow cuts sting intensely because superficial dermal nerve endings are more reactive when exposed. A breached epidermal surface leaves local nociceptors raw and open to repeated restimulation from the environment.
What are superficial dermal nerve endings?
Superficial dermal nerve endings are free nerve endings located primarily in the papillary dermis. They function as fast-acting nociceptors that detect damaging mechanical, thermal, and chemical stress at the skin’s surface.
Why does air make a superficial wound hurt more?
Air makes a superficial wound hurt more because evaporative cooling and drafts repeatedly stimulate exposed nerve endings. This continuous environmental contact causes the A-delta fibers to keep firing sharp pain signals.
Why do fingertip wounds feel especially sharp?
Fingertip wounds feel especially sharp because the fingertips are a densely innervated region. The high concentration of free nerve endings amplifies local nociceptor reactivity, producing a stronger neural alarm signal.
Do deeper wounds always hurt more than superficial ones?
No. Deeper wounds often destroy the pain-sensing free nerve endings completely, muting the immediate sharp stinging response, whereas superficial wounds leave millions of intact, irritated nerve endings continuously exposed.
What kind of dressing reduces stinging pain fastest?
Occlusive coverage, such as a hydrocolloid dressing, reduces stinging pain rapidly by insulating the exposed nerve endings. This physical barrier completely blocks the airflow and friction that trigger repeated restimulation.
Do topical anesthetics help reactive superficial wounds?
Yes, topical anesthetics like lidocaine help reactive superficial wounds by temporarily blunting local nerve firing. They stop the localized overfiring of nociceptors, making the stinging pain much easier to tolerate.
Conclusion
In conclusion, superficial dermal nerve endings are more reactive because their surface-near position makes them easier to expose, easier to restimulate, and more likely to generate sharp pain after shallow injury.
By understanding that dense sensory zones and raw exposure trigger rapid nociceptor firing, it becomes clear why shallow wounds sting so sharply. Treating this reactivity effectively relies on insulating the breach and blunting local nerve firing, successfully protecting the skin while it repairs.