
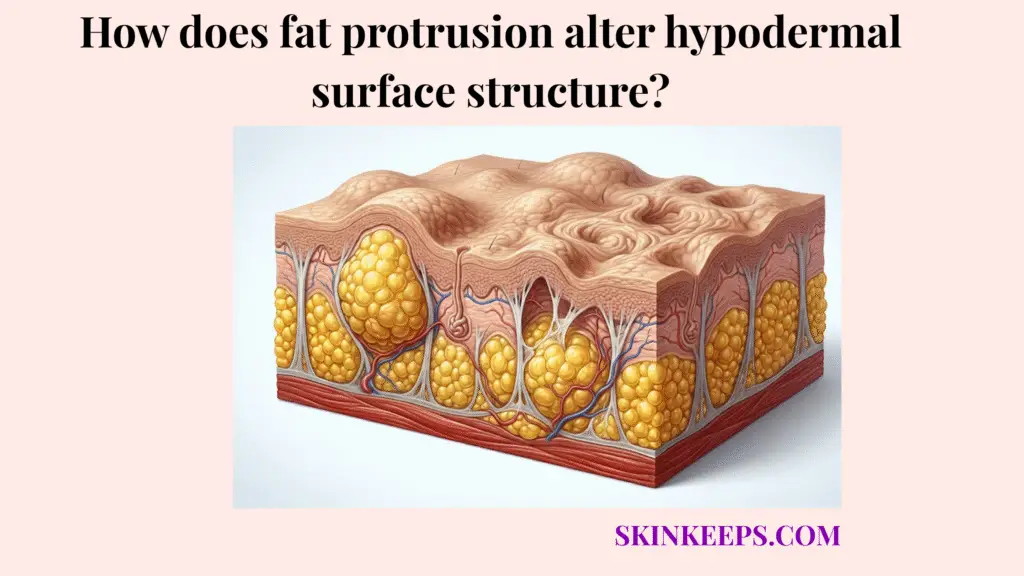
Hypodermal fat protrusion alters skin surface structure when enlarged or poorly supported fat lobules press upward against the dermis, creating visible bumps, dimples, or uneven texture at the surface. This structural skin change relies heavily on the physiological balance between connective tissue restraint and upward adipose pressure.
This clinical guide covers how these structural factors permanently alter tissue architecture and visible skin smoothness. It explains the mechanics behind adipose herniation, the role of dermal support, and the realistic treatment categories available.
What exactly is hypodermal fat protrusion and how does it compromise skin smoothness?
Hypodermal fat protrusion compromises skin smoothness when subcutaneous fat lobules press upward across the dermal-fat boundary and create uneven pressure beneath the skin surface. This upward shift pushes the delicate overlying structures out of their normal, flat alignment.
When this underlying tissue architecture shifts, the normally smooth dermal boundary distorts. This distortion visually alters the skin envelope, making internal fat compartment expansion apparent on the outside.
How does adipose herniation change hypodermal structure?
Adipose herniation changes hypodermal structure when fat lobules bulge upward toward the dermis instead of remaining evenly supported within their subcutaneous compartments. This localized bulging disrupts the natural equilibrium of the subcutaneous layer.
Cellulite affects approximately 80–90% of postpubertal women, which supports framing adipose protrusion patterns as common structural skin findings rather than rare abnormalities. [PubMed]
How does disruption of the dermal-fat boundary alter skin texture?
Disruption of the dermal-fat interface alters skin texture because the normally smooth transition between dermis and hypodermis becomes uneven when fat lobules press upward irregularly. This uneven boundary translates directly into wavelike or distorted surface contours.
As the interface loses its flat configuration, the overlying skin mimics the irregular shape below. This disrupted structural support ultimately reveals itself as visible surface irregularities or pronounced bumps.
Why does the upward push of enlarged adipocytes create visible surface irregularities?
The upward push of enlarged adipocytes creates visible surface irregularities because expanded fat cells increase pressure inside subcutaneous compartments and press unevenly against the overlying dermis. This outward tissue pressure forces the dermal layer to stretch and warp.
As the adipocytes grow, they consume the limited space within their connective boundaries. This localized adipose bulging then forces the tissue to compensate by pushing the skin outward.
How does adipocyte hypertrophy increase upward pressure?
Adipocyte hypertrophy increases upward pressure when fat cells enlarge through lipid storage and occupy more space within the same subcutaneous tissue compartment. This triglyceride storage physically expands the entire cellular matrix.
The swollen fat lobules then press aggressively against the skin’s undersurface. If the overlying dermis cannot resist this force, the outward pressure creates a localized, visible bump.
How can connective tissue restraints shape protruding fat?
Connective tissue restraints shape protruding fat by limiting where expanded fat lobules can move, which can make upward pressure appear as localized bumps or dimples. Fibrous septae act as rigid walls that prevent the fat from spreading laterally.
Because the fat cannot move sideways, it is forced to bulge upward between these restrictive bands. This localized protrusion creates the undulating, uneven surface characteristic of many hypodermal irregularities.
| Anatomical State | Internal Pressure | Dermal Boundary Status | Visible Surface Result |
|---|---|---|---|
| Evenly supported fat | Balanced pressure inside compartments | Smooth dermal-fat boundary | Even skin surface |
| Enlarged adipocytes | Greater compartment pressure | Mild upward pressure on dermis | Subtle uneven texture |
| Protruding fat lobules | Uneven upward pressure | Wavelike dermal-fat boundary | Bumps, dimples, or irregularity |
| Weak dermal roof | Less resistance above protruding fat | Boundary becomes more visible | Surface texture appears more pronounced |
| Tight fibrous septae | Fat bulges between fixed bands | Alternating pull and push | Dimpled cellulite-like pattern |
How does a thinning dermal roof amplify the appearance of protruding subcutaneous lobules?
A thinning dermal roof amplifies the appearance of protruding subcutaneous lobules because weaker collagen and elastin support makes the overlying skin less able to hide uneven pressure from below. This reduced skin envelope strength allows the internal irregularities to project outwardly.
When the reticular dermis loses its structural density, it functions less like a sturdy shield and more like a fragile veil. Consequently, normal subdermal fat compartments become instantly more visible at the surface.
Why does dermal thickness control how visible fat protrusion becomes?
Dermal thickness controls how visible fat protrusion becomes because a stronger collagen-rich dermis can buffer minor unevenness, while a thinner dermis reveals more of the texture beneath it. This dermal resistance essentially masks the underlying adipose tissue pressure.
Tretinoin treatment produced an 80% increase in collagen I formation compared with a 14% decrease with vehicle in photodamaged skin, which supports the idea that dermal collagen biology can be modified, although this does not prove cellulite correction. [PubMed]
How does collagen degradation reduce resistance to upward fat pressure?
Collagen degradation reduces resistance to upward fat pressure because collagen normally gives the dermis tensile strength that helps maintain a smoother surface over subcutaneous fat. When this collagen network fragments, the reticular dermis support weakens significantly.
Without strong structural fibers to hold it back, the dermal-fat interface yields easily to the outward-pushing lipid matrix. This structural failure guarantees that even minor fat expansion becomes highly visible.
Which metabolic factors accelerate localized bulging of the adipose layer?
Metabolic factors may accelerate localized bulging of the adipose layer by increasing lipid storage, fluid retention, tissue swelling, or compartment pressure inside subcutaneous fat lobules. These systemic shifts directly impact how much physical space the fat occupies.
By altering the internal volume of the hypodermis, these factors exacerbate existing structural weaknesses. Careful metabolic volume control may therefore help mitigate the severity of visible skin texture distortion.
How can hyperinsulinemia and lipid storage influence adipose protrusion?
Hyperinsulinemia and lipid storage may influence adipose protrusion because insulin supports fat storage pathways, and larger adipose compartments can press more visibly against the dermis. This insulin-related lipogenesis directly expands the cells within the hypodermis.
As the fat lobules increase in size, they apply greater mechanical stress against the dermal barrier. This increased compartment pressure makes structural fat herniation much more visually pronounced.
How can edema and interstitial fluid retention amplify surface bumps?
Edema and interstitial fluid retention can amplify surface bumps because extra fluid increases tissue volume around fat lobules and makes uneven pressure more visible at the skin surface. This fluid-related swelling fills the tight spaces between adipocytes.
The trapped interstitial fluid adds supplementary outward pressure against the already strained dermal roof. Consequently, poor microvasculature or lymphatic drainage may make the undulating dermal border appear significantly worse.
What myths should be avoided when trying to flatten structural fat herniation?
Myths should be avoided when trying to flatten structural fat herniation because surface-level methods cannot reliably shrink deep adipocytes, release fibrous septae, or rebuild the dermal support layer. The skincare market often promotes superficial fixes for these deeply architectural problems.
Believing that scrubs or lotions can cure deep tissue bulging only leads to frustration. Effective management requires differentiating temporary smoothing from actual structural correction.
Why can’t topical creams shrink hypertrophic fat cells?
Topical creams cannot reliably shrink hypertrophic fat cells because most over-the-counter products act on the skin surface rather than directly reducing the volume of deep subcutaneous adipocytes. They simply cannot penetrate deeply enough to empty lipid stores.
AAD states that cellulite creams cannot remove cellulite permanently, which supports separating temporary surface changes from true structural correction. [AAD]
Why does muscle toning not directly stop fat lobule protrusion?
Muscle toning does not directly stop fat lobule protrusion because exercise strengthens the muscle beneath the fat layer, while protrusion depends on adipose volume, dermal support, and connective tissue architecture. Building muscle improves overall body composition but does not release structural tethers.
This spot reduction myth assumes that muscle work directly flattens the overlying fat compartments. While fitness supports tissue health, it cannot selectively erase a protruding subcutaneous lobule.
Which clinical procedures may reduce or mask the appearance of an outward-pushing lipid matrix?
Clinical procedures may reduce or mask the appearance of an outward-pushing lipid matrix by either reducing focal fat volume, remodeling dermal support, or strengthening the skin envelope above protruding lobules. These methods bypass surface myths to address actual tissue mechanics.
A clinician-guided treatment plan ensures the right technology targets the specific layer causing the surface irregularity. Choosing the correct intervention is vital for safe and realistic appearance improvement.
Which procedures reduce the push by targeting fat volume?
Procedures that reduce the push by targeting fat volume include focal fat reduction methods such as cryolipolysis, radiofrequency-based contouring, or laser treatment selected by a qualified clinician. These technologies aim to physically decrease the size of the offending fat compartments.
Cryolipolysis studies have reported subcutaneous fat reduction up to 25% after one treatment, which supports describing it as a focal fat-reduction method rather than a direct cellulite cure. [PMC]
Which procedures strengthen the dermal roof over protruding fat?
Procedures that strengthen the dermal roof over protruding fat include collagen-supporting strategies such as radiofrequency, laser resurfacing approaches, retinoids, or biostimulatory fillers used for selected patients. These interventions focus strictly on a skin-thickening strategy rather than volume removal.
By enhancing collagen density, these treatments help the skin envelope better resist underlying fat pressure. A review of collagen stimulators in body applications notes their expanding use for concerns including skin laxity, cellulite, striae, and wrinkles, supporting cautious discussion of biostimulatory fillers as collagen-support strategies rather than fat-reduction procedures. [PMC]
| Procedure | Targets Fat or Skin? | Mechanism of Action | Visual Surface Result |
|---|---|---|---|
| Cryolipolysis | Fat volume | Cooling-induced focal fat reduction | May reduce localized fullness |
| Radiofrequency contouring | Fat and/or dermis depending on device | Heat-based remodeling | May improve contour or firmness |
| Laser-assisted treatment | Fat, dermis, or septae depending on system | Energy-based remodeling | May improve texture in selected patients |
| Biostimulatory fillers | Dermal support | Collagen-stimulating volume/support | May camouflage shallow irregularities |
| Retinoids | Dermal biology | Collagen-supporting skin care | May support dermal resilience over time |
| Topical firming creams | Skin surface | Temporary hydration or tightening | Temporary appearance change only |
| Exercise and nutrition | Metabolic/tissue support | Body composition and tissue health | Supportive, not direct protrusion release |
What daily checklist helps manage the surface impact of deep tissue bulging?
A daily checklist helps manage the surface impact of deep tissue bulging by supporting metabolic stability, reducing fluid-related swelling, protecting dermal collagen, and avoiding unrealistic spot-reduction claims. Consistent, low-impact daily habits preserve the integrity of the dermal-fat interface.
This supportive routine emphasizes realistic volume management over aggressive, ineffective cosmetic fixes. Following these steps helps maintain long-term skin health.
How can metabolic volume control reduce surface irregularity?
Metabolic volume control can reduce surface irregularity by supporting stable energy storage, limiting avoidable fluid retention, and reducing swelling that can make protruding fat lobules look more visible. Stable blood sugar limits the aggressive expansion of fat compartments.
Additionally, moderating sodium intake minimizes the interstitial fluid that adds unnecessary outward pressure. Together, these habits subtly reduce the physical push against the dermis.
How can dermal fortification habits support the skin envelope?
Dermal fortification habits can support the skin envelope by protecting collagen from UV damage and using well-tolerated topical strategies that may improve dermal resilience over time. Applying daily SPF preserves the vital structural proteins that hold the skin tight.
Tretinoin treatment produced an 80% increase in collagen I formation compared with a 14% decrease with vehicle in photodamaged skin, but this should be framed as dermal collagen biology rather than proof of cellulite correction. [PubMed]
Daily Hypodermal Volume & Surface Management Checklist
FAQs About Fat Protrusion and Hypodermal Surface Structure
Is hypodermal fat protrusion the same as weight gain?
No. Hypodermal fat protrusion describes how fat lobules press upward against the dermis and alter surface texture. Weight gain can increase fat volume, but visible protrusion also depends on connective tissue restraint, dermal thickness, and the smoothness of the dermal-fat boundary.
Why does fat protrusion create bumps or dimples?
Fat protrusion creates bumps or dimples when enlarged or unevenly supported fat lobules push upward while fibrous septae and dermal support create uneven resistance. The surface change comes from tissue architecture, not from fat volume alone.
How common are cellulite-like protrusion patterns?
Cellulite is very common in postpubertal women. Evidence reviews describe cellulite as present in approximately 80–90% of postpubertal women, which supports framing fat protrusion and surface irregularity as common structural patterns rather than rare abnormalities.
Can creams shrink protruding fat cells?
No topical cream can reliably shrink deep adipocytes or empty lipid stores inside subcutaneous fat lobules. Some products may temporarily improve hydration, firmness, or texture, but they should not be framed as structural fat-reduction treatments.
Does exercise stop fat lobules from protruding?
Exercise can improve muscle tone, circulation, and body composition, but it does not directly release fibrous septae or specifically flatten one protruding fat lobule. It should be framed as supportive tissue care, not a spot-reduction cure.
Which treatments target the fat-volume side of protrusion?
Fat-volume treatments include clinician-guided options such as cryolipolysis, radiofrequency-based contouring, or laser-assisted approaches. Cryolipolysis studies in one review reported fat reduction up to 25% after one treatment, but results vary and do not guarantee cellulite correction.
Which treatments target the dermal-support side?
Dermal-support treatments include retinoids, radiofrequency, laser approaches, and biostimulatory fillers in selected patients. These strategies aim to support the skin envelope above protruding fat, not remove fat lobules directly.
Conclusion
Hypodermal fat protrusion alters surface structure by creating upward pressure from fat lobules while dermal thickness, collagen support, and fibrous septae determine how visible that pressure becomes. This delicate interplay means that surface bumps are rarely just an issue of excess weight, but rather a complex architectural challenge within the subcutaneous layer.
Metabolic swelling, fluid retention, and degraded collagen all amplify these structural irregularities. At SkinKeeps, we explain skin structure through evidence-based dermatology so readers can understand visible surface changes without shame, exaggeration, or false treatment promises.
Understanding fat protrusion as a structural interaction between adipose volume, dermal support, and connective tissue restraint helps readers choose realistic care with clarity and confidence.



