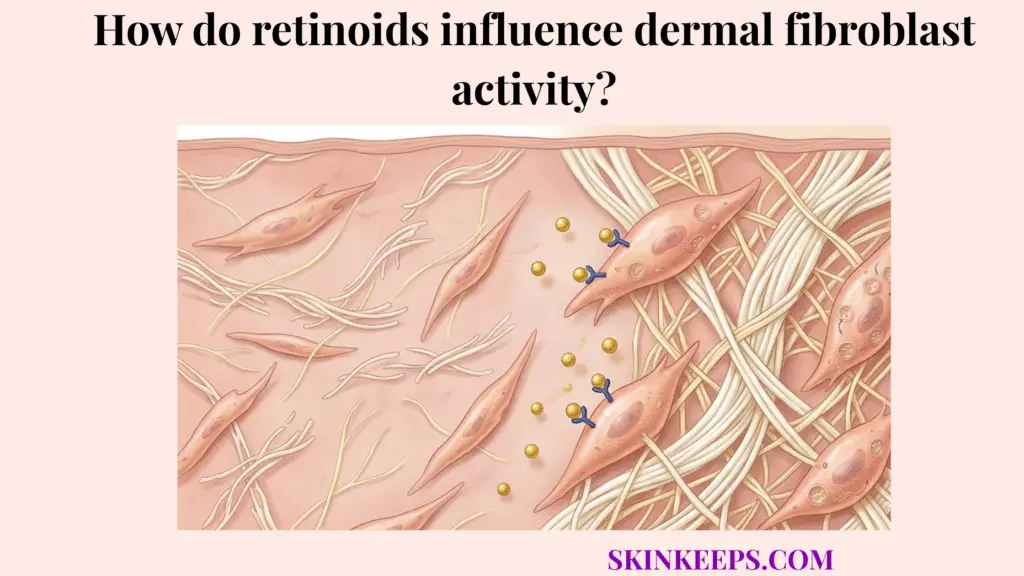
Retinoids influence dermal fibroblast activity by changing the signaling environment that controls collagen production, matrix repair, and dermal remodeling. When fibroblasts respond to retinoid signaling, they can shift toward stronger collagen-supportive behavior and a more organized repair pattern over time.
It is important to recognize that retinoids are not just surface-renewal ingredients. While they do accelerate epidermal cell turnover to provide a smoother texture, their profound clinical value lies much deeper. They penetrate the skin’s outer shield (the epidermis) to directly interface with the living factories of the dermis, actively reprogramming how the skin builds and maintains its structural scaffolding.
Understanding exactly how retinoids influence dermal fibroblast activity requires mapping the biological baseline, tracking receptor signaling to gene regulation, evaluating the balance between collagen synthesis and degradation, comparing prescription and cosmetic forms, and defining the supportive habits that preserve the final remodeling result.
What is the biological baseline for how retinoids influence dermal fibroblast activity?
The biological baseline is that fibroblasts are the main dermal cells responsible for producing collagen and maintaining extracellular matrix quality, so any treatment that changes fibroblast behavior can change long-term dermal structure.
Dermal fibroblasts act as the central architects of the skin. They continuously synthesize the structural proteins—collagen and elastin—that give the dermis its firmness, tensile strength, and resilient bounce.
Fibroblast-focused skin-aging reviews explicitly frame dermal fibroblasts as a main anti-aging target because collagen support, matrix maintenance, and structural resilience depend heavily on them. If a topical ingredient cannot communicate with these specific cells, it cannot produce true structural remodeling. (PMC)
Semantic Profile
- 1. Fibroblasts maintain the collagen-rich dermal matrix.
- 2. Disrupted fibroblast behavior weakens structure.
- 3. Treatments that normalize fibroblasts can improve dermal remodeling.
How does retinoid receptor signaling explain how retinoids influence dermal fibroblast activity?
Retinoid receptor signaling explains the mechanism because retinoids regulate gene transcription by binding to nuclear retinoid receptors, especially RARs and RXRs, which then alter how target cells interpret repair and remodeling instructions.
When retinoic acid enters the dermis, it bypasses the cell membrane and enters the fibroblast directly. Once inside, it binds to Retinoic Acid Receptors (RAR) and Retinoid X Receptors (RXR) located in the cell nucleus.
That receptor-driven transcriptional control is the first reason retinoids can influence fibroblasts at a deeper biologic level rather than acting only as superficial exfoliants. They act as molecular keys that physically unlock specific genetic sequences related to structural repair. (PMC)
Semantic Profile
- 1. Retinoid reaches target tissue.
- 2. RAR/RXR signaling changes transcriptional instructions.
- 3. Fibroblast behavior shifts over time.
How does gene regulation explain how retinoids influence dermal fibroblast activity?
Gene regulation explains the effect because once retinoid signaling begins, fibroblast gene-expression patterns can shift toward more extracellular-matrix support and less photoaging-associated dysfunction.
When the RAR/RXR receptors are activated, they prompt the fibroblast to upregulate the genes responsible for producing healthy structural proteins while downregulating the genes that drive destructive inflammatory enzymes, such as Matrix Metalloproteinases.
Recent retinol-focused work specifically highlights upregulation of the TGF-β/CTGF pathway in aged human skin, which is directly relevant to matrix support and fibroblast behavior. By regulating these specific pathways, retinoids act as powerful directors of cellular behavior. (PMC)
Semantic Profile
- 1. Retinoid receptor signaling changes gene-expression programs.
- 2. Fibroblasts receive more matrix-supportive instructions.
- 3. Dermal remodeling becomes more favorable.
How do retinoids influence dermal fibroblast activity toward collagen synthesis?
Retinoids influence dermal fibroblast activity toward collagen synthesis by shifting fibroblasts into a more collagen-supportive state, which is especially relevant in photoaged skin where collagen support has become weaker, leading to a decrease in dermal collagen density.
Once the genes are activated, the fibroblast significantly ramps up its production of procollagen, the precursor molecule that is eventually assembled into strong collagen fibers outside the cell. Reviews of cosmetic retinoids and tretinoin both state that retinoids can activate new collagen synthesis by dermal fibroblasts.
A classic photodamage study, as cited in later retinoid reviews, found that topical tretinoin increased type I collagen production by about 80% in photoaged skin compared to vehicle controls. This is one of the clearest numeric anchors for why retinoids are treated as genuine dermal collagen-supportive agents rather than mere exfoliants. (Tretinoin Peel: A Critical View / PMC)
How do retinoids influence dermal fibroblast activity against collagen degradation?
Retinoids affect collagen balance, not just collagen production. Retinoid reviews report that retinoids can reduce MMP activity (Matrix Metalloproteinases, the enzymes that break down collagen) while increasing inhibitors of collagen degradation.
Skin health is a constant battle between production and destruction. UV exposure generates excessive MMPs, which act like biological scissors chopping up the collagen matrix. Retinoids aggressively suppress the expression of these destructive enzymes.
This means their dermal effect is better framed as restoring collagen balance than simply “adding collagen.” They help rebuild the wall while stopping the demolition crew from tearing it down.
How do retinoids influence dermal fibroblast activity in photoaged skin versus healthier skin?
Retinoids influence dermal fibroblast activity more noticeably in photoaged skin because fibroblast behavior in damaged dermis is more disrupted and therefore has more to correct.
Photoaged fibroblasts (cells chronically damaged by UV exposure) are biologically sluggish. Fibroblast-aging reviews describe them as structurally and functionally impaired. Their collagen output is drastically reduced, and they constantly produce excess destructive MMPs. This helps explain why retinoid-driven normalization is especially relevant there.
In younger, healthier skin, fibroblasts are already operating efficiently, so the visible difference from retinoid use is less dramatic and functions more as a preventative preservation strategy.
| Dermal state | Fibroblast behavior | Collagen-support quality | Structural outcome |
|---|---|---|---|
| Healthier dermis | More balanced | Better maintained | More stable structure |
| Photoaged dermis | More disrupted | Lower or disorganized | Weaker matrix support |
| Retinoid-supported photoaged dermis | More normalized over time | Improved collagen-support tendency | Gradual remodeling improvement |
How do prescription and cosmetic forms differ in how retinoids influence dermal fibroblast activity?
Prescription and cosmetic forms differ because prescription-strength retinoids usually produce stronger and more predictable biologic effects, whereas cosmetic retinol and related forms can still influence fibroblast activity but often with milder, slower, and more formulation-dependent results.
Retinoic acid (tretinoin) is biologically active immediately. When it touches a fibroblast, it binds directly to the RAR/RXR receptors to initiate gene regulation.
Cosmetic retinol and retinaldehyde must undergo a biochemical conversion process within the skin to become retinoic acid. This conversion reduces the sheer volume of active molecules available to the cell. Broad retinoid reviews and dermatologist guidance both support this hierarchy: prescription retinoids provide the most intense remodeling, while cosmetic forms provide a gentler, more gradual approach with less initial irritation.
How long does it take before how retinoids influence dermal fibroblast activity becomes visible?
Visible structural change from fibroblast-directed retinoid remodeling is delayed because fibroblast-driven collagen support is slower than surface turnover changes.
While you may experience smoother texture or an epidermal “glow” within a few weeks due to faster surface shedding, true dermal remodeling is a slow, structural process. Generating new procollagen, assembling it into rigid fibers, and organizing the extracellular matrix takes months.
Retinoid reviews consistently describe dermal improvement as gradual, with clinical and histologic changes developing over sustained use rather than over days.
What limits how retinoids influence dermal fibroblast activity?
Retinoid-driven fibroblast remodeling is limited by age, chronic UV exposure, smoking-related vascular stress, metabolic burden, poor tolerance, and inconsistent use.
Retinoids are not magic. They are signaling molecules. If a fibroblast is starved of oxygen due to smoking, heavily mutated by severe sun damage, or if the patient cannot tolerate the product and constantly stops applying it, the remodeling signal will fail.
Fibroblast-centered aging literature and photoaging reviews both support the idea that the repair environment can either support or blunt long-term structural improvement. If the skin is kept in a state of severe inflammation, the retinoids cannot overcome the biological ceiling of the damaged tissue.
What supportive habits improve how retinoids influence dermal fibroblast activity?
Supportive habits improve the fibroblast response because daily photoprotection, barrier stability, and consistent tolerable use protect retinoid-driven remodeling from being undone by ongoing UV damage and irritation.
Without broad-spectrum sunscreen, daytime UV rays will trigger MMP enzymes that shred the exact collagen fibers the retinoids stimulated the fibroblasts to build the night before. Understanding how UV radiation degrades dermal collagen explains why avoiding this damage is crucial. Reviews of photoaging and antiaging care consistently place daily sunscreen and combined retinoid-antioxidant-photoprotection strategies at the center of long-term results. (PMC)
What steps can you take today if you want how retinoids influence dermal fibroblast activity to work better?
The best practical approach is to combine daily broad-spectrum sun protection, retinoid use at a tolerable frequency, barrier support that preserves consistency, and realistic long-term expectations. Dermatologist guidance also supports starting with lower frequency and building up rather than trying to force fast results through irritation (American Academy of Dermatology).
Final Execution Checklist
What are the key summary facts about how retinoids influence dermal fibroblast activity?
The key summary facts are that retinoids influence dermal fibroblast activity through receptor signaling and downstream gene regulation, that their effects include more collagen-supportive behavior and better matrix-remodeling balance, and that the final outcome depends on consistency, UV control, tissue condition, and time.
Summary Points
Quick Answers About How Retinoids Influence Dermal Fibroblast Activity
What do retinoids actually do to fibroblasts?
Retinoids change the signaling and gene-expression environment that fibroblasts follow, pushing them toward more collagen-supportive and matrix-repair behavior over time.
Do retinoids only exfoliate the skin surface?
No. Their deeper value comes from receptor-mediated effects that influence dermal biology, including fibroblast-related remodeling, not just superficial turnover.
Do retinoids increase collagen or only prevent collagen loss?
They appear to do both. Reviews report activation of new collagen synthesis by dermal fibroblasts and reduction of MMP activity linked to matrix breakdown.
Why do retinoids matter more in photoaged skin?
Because photoaged fibroblasts are more disrupted, so there is more dysfunctional matrix behavior to correct and normalize.
Is tretinoin stronger than cosmetic retinol?
Usually yes. Prescription-strength retinoids are generally more potent and more predictable, while cosmetic retinol is usually milder and more formulation-dependent.
How long before fibroblast-related improvement becomes visible?
It is gradual. Surface changes may appear earlier, but meaningful dermal remodeling and collagen-supportive change take sustained use over time.
Can irritation make retinoids work faster?
Not in any reliable way. Excess irritation can destabilize tolerance and make long-term consistent use harder, which undermines remodeling progress.
Why is sunscreen so important if I already use retinoids?
Because UV exposure counteracts retinoid-driven dermal progress and remains a major driver of photoaging. Daily photoprotection helps preserve any collagen-supportive gains.
Do antioxidants help retinoid-driven fibroblast remodeling?
They can help support the environment by reducing oxidative stress and complementing broader anti-photoaging strategies, but they are not the same thing as direct retinoid signaling.
What is the best routine mindset for retinoid remodeling?
Think in months, not days: protect from UV, keep the barrier stable, use retinoids consistently at a tolerable level, and avoid judging progress by early peeling alone.
Conclusion
In conclusion, retinoids influence dermal fibroblast activity through RAR/RXR-driven signaling and downstream gene regulation that shift fibroblasts toward more collagen-supportive, matrix-repair, and photoaging-corrective behavior over time.
That is why their value extends beyond exfoliation: they act on the cells that help maintain dermal structure itself. But those gains remain gradual, conditional, and strongly dependent on consistency, tissue condition, and daily photoprotection.