
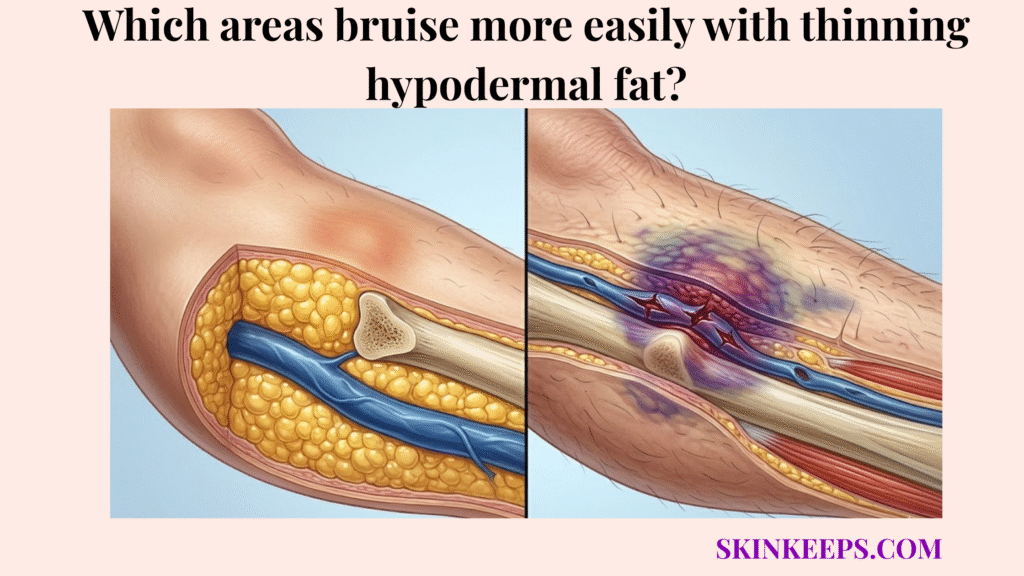
Thinning hypodermal fat makes the dorsal hands, extensor forearms, shins, lower legs, and periorbital region more prone to bruising because these zones have less protective padding, more mechanical exposure, or thinner skin over fragile superficial vessels. This structural support loss transfers everyday mechanical stress directly into local capillaries.
The hypodermis provides essential subcutaneous padding, but this cushioning naturally diminishes over time. This guide explains regional bruising susceptibility, local tissue weaknesses, and safe physical protection strategies. Any unusual, sudden, or painful bruising requires a clinician review to ensure overall medical safety.
Why do specific anatomical regions bruise faster with depleted subcutaneous padding?
Specific anatomical regions bruise faster with depleted subcutaneous padding because fat loss does not create equal mechanical risk across the body; areas with thin baseline padding, high friction, sun exposure, or close bone support become vulnerable first. This regional bruising susceptibility dictates where visible injury naturally clusters. Consequently, trauma patterns clearly follow these local anatomical weaknesses.
For example, limbs experience more daily contact than the central trunk. When age or photodamage reduces the soft-tissue buffer, these specific anatomical regions cannot dissipate kinetic energy. This failure allows minor surface impacts to reach and rupture underlying capillaries easily.
How does uneven fat atrophy create regional bruising susceptibility?
Uneven fat atrophy creates regional bruising susceptibility because each body zone begins with a different amount of soft-tissue padding, friction exposure, and vascular support. This baseline inequality means that as overall fat diminishes, naturally leaner areas become mechanically fragile sooner. The extensor surfaces often exhibit this vulnerability because they endure frequent bumps alongside heavy sun damage.
This combined mechanical and environmental stress makes vascular rupture highly visible. Senile purpura affects over 10% of people aged over 50 years, which shows why regional bruising on sun-exposed older skin is clinically common [DermNet].
Why does skin close to bone or tendon bruise more easily?
Skin close to bone or tendon bruises more easily because a smaller soft-tissue buffer leaves superficial vessels with less protection when pressure is applied from the outside. Without deep fat to absorb the compression, vessels are quickly crushed against the rigid bone. This low-buffer vulnerability explains why minor trauma frequently produces persistent discoloration.
The back of the hand and the anterior shin lack substantial fat padding even in healthy youth. DermNet describes senile purpura lesions as irregular macules measuring 1–4 cm in diameter and taking up to 3 weeks to resolve [DermNet].
| Body Zone | Local Vulnerability | Main Mechanical Trigger | Visible Pattern |
|---|---|---|---|
| Dorsal hands | Thin padding and high sun exposure | Minor bumps and shearing force | Purple macules/ecchymoses |
| Extensor forearms | Sun damage plus frequent contact trauma | Desk pressure, door bumps, reaching | Actinic/senile purpura |
| Shins / anterior tibia | Skin lies close to bone with limited soft-tissue buffer | Table edges, car doors, falls | Larger bruises or hematomas |
| Lower legs | Gravity and vascular pressure may worsen swelling or bleeding visibility | Standing, trauma, vascular disease | Persistent discoloration or hematoma |
| Periorbital region | Very thin skin and little/no subcutaneous fat in eyelids | Eye rubbing, minor trauma, edema | Dark discoloration or visible bruising |
Why are the dorsal hands and forearms most susceptible to vascular rupture from diminished deep fat?
The dorsal hands and extensor forearms are most susceptible to vascular rupture from diminished deep fat because they combine thin soft-tissue padding, frequent minor trauma, and high cumulative sun exposure. This distinct double-hit mechanism severely undermines the local vascular support network. Consequently, these locations represent the most recognizable sites for structural bruising.
When daily actions involve reaching or resting arms on firm surfaces, the compromised tissue repeatedly fails to absorb the pressure. Actinic purpura frequently emerges in these zones due to this repetitive mechanical strain. The superficial capillaries simply lack the foundational architecture needed to survive everyday friction.
Why does the dorsal hand and forearm vascular network become exposed?
The dorsal hand and forearm vascular network becomes more exposed when subcutaneous padding and dermal support decline, leaving superficial vessels less protected from repeated contact and shearing force. This loss of support allows the vascular structures to rest closer to the delicate skin surface. Because these vessels sit in a depleted matrix, lateral pulling or direct compression easily tears their walls.
This exposure creates a highly visible bleeding pattern following minor trauma. DermNet reports that senile purpura affects over 10% of people aged over 50 years, and its lesions are most commonly distributed on the extensor forearms and dorsal hands [DermNet].
How does UV damage create a double-hit on forearm bruising?
UV damage creates a double-hit on forearm bruising because chronic sun exposure weakens dermal collagen while age-related padding loss reduces the mechanical cushion beneath the same vessels. This combined degradation destroys the entire three-dimensional support system surrounding the capillaries. As a result, collagen degradation fundamentally amplifies the mechanical weakness caused by missing fat.
This photodamage explains why these specific, sun-exposed surfaces bruise so easily compared to protected trunk skin. StatPearls estimates actinic purpura is present in about 12% of individuals older than 50 and 30% of those aged 75 and older, making sun-exposed forearm bruising a common aging-skin pattern [NCBI].
How does a shrinking adipose buffer increase bruising risk on the shins and lower legs?
A shrinking adipose buffer increases bruising risk on the shins and lower legs because these areas often have less soft-tissue protection over firm underlying structures and are exposed to frequent low-level trauma. The anterior tibia rests directly beneath the skin, offering minimal mechanical defense against physical impact. This bone-proximity vulnerability guarantees that even low-energy bumps transfer intense pressure directly into local vessels.
When the pretibial region loses its remaining subcutaneous fat, it loses its only shock absorber. Consequently, larger bruises or hematomas may occur easily upon encountering daily obstacles like furniture edges or car doors. Any expanding hematoma or severe pain in these vulnerable lower zones requires careful clinician review to ensure proper healing.
Why is the anterior tibial region vulnerable to bruising?
The anterior tibial region is vulnerable to bruising because the skin over the shin has limited soft-tissue buffering between the surface and the underlying tibia. This lack of deep padding traps the superficial blood vessels against the rigid bone during any blunt contact. The resulting localized compression quickly ruptures the unsupported capillaries.
Pretibial injuries in older adults are often linked to minor low-energy trauma, and one review notes that pretibial injuries affect roughly 0.4–0.7 per 1000 people per year, with pretibial hematomas complicating 42% of pretibial injuries admitted for hospital treatment [Journal on Surgery].
How do gravity and hydrostatic pressure affect lower-leg bruising?
Gravity and hydrostatic pressure can affect lower-leg bruising by increasing fluid and vascular pressure in dependent tissues, which may make bleeding, swelling, or discoloration more persistent after trauma. Because the lower legs support the body’s fluid column during standing, local venous pressure naturally rises. This pressure places additional functional stress on blood vessels that already lack structural cushioning.
When trauma occurs, this hydrostatic pressure can exacerbate blood leakage, enlarging the visible ecchymoses. The presence of underlying vascular disease or anticoagulant use may further prolong this tissue discoloration. For this reason, utilizing compression therapy to manage dependent fluid must always remain clinician-guided.
Why does the periorbital region become prone to mechanical fragility as facial fat pads thin?
The periorbital region becomes prone to mechanical fragility as facial fat pads thin because eyelid skin is extremely thin and has very little soft-tissue buffering over delicate vessels. This distinct local anatomy relies heavily on underlying orbital fat support. When this regional volume diminishes, the microvascular network sits exceptionally close to the surface.
This structural change increases visible vulnerability to microtrauma. Daily habits like aggressive eye rubbing apply shearing force directly to these unprotected vessels, which may worsen dark discoloration. However, any sudden periorbital bruising lacking clear trauma must be medically evaluated to rule out serious conditions.
How does facial fat pad thinning change under-eye support?
Facial fat pad thinning changes under-eye support by reducing the soft-tissue volume that normally smooths the transition between the lower eyelid and the cheek. The sub-orbicularis oculi fat provides essential structural backing for this highly delicate area. As this supportive volume changes, a hollowed appearance often exposes the underlying vascular shadowing.
This loss of localized padding leaves the thin periorbital tissue mechanically fragile. NCBI Bookshelf describes eyelid skin as having no subcutaneous fat and being the thinnest layer of skin on the body, which explains why the periorbital region shows vascular and pigment changes easily [NCBI].
Why does thin eyelid skin show microtrauma more easily?
Thin eyelid skin shows microtrauma more easily because its limited soft-tissue buffering allows small changes in blood, pigment, fluid, or shadowing to become visible at the surface. Friction from rubbing allergic or irritated eyes can quickly rupture unprotected micro-vessels. This repetitive friction creates visible discoloration that mimics deep bruising.
Because the epidermis here provides negligible camouflage, leaked blood readily stains the tissue. If periorbital bruising appears spontaneously, or is accompanied by vision changes or severe swelling, immediate medical care is necessary. Avoiding habitual eye rubbing is a fundamental protective strategy for this delicate zone.
Which localized stressors accelerate bleeding in areas with reduced biological cushioning?
Localized stressors accelerate bleeding in areas with reduced biological cushioning by adding friction, pressure, UV exposure, or chemical irritation to skin that already has less mechanical support. Thin padding reduces the trauma threshold, meaning everyday environmental factors easily trigger vessel leakage. Identifying these localized stressors is critical for preventing persistent discoloration.
These external factors apply shearing force or compromise tissue integrity further. For example, aggressive skincare routines or constrictive fabrics physically tear unprotected capillaries. Recognizing these specific friction points allows patients to implement low-friction handling and protect their most vulnerable skin zones.
How do friction and restrictive clothing worsen high-risk bruising zones?
Friction and restrictive clothing worsen high-risk bruising zones because repeated rubbing and pressure increase shearing force across thin, poorly cushioned skin. Tight elastic bands on forearms or lower legs can mechanically pull the fragile epidermis laterally. This lateral stress directly transfers to the unanchored capillaries underneath.
Because depleted padding cannot absorb this lateral pull, the vessels may tear. Wearing loose, non-abrasive fabrics may help protect fragile skin from this repeated mechanical shear. Avoiding constrictive garments is a simple, effective method to reduce localized bruising risks.
Why can aggressive topical application damage fragile regional skin?
Aggressive topical application can damage fragile regional skin because rubbing creams into thin forearms, shins, or eyelids adds mechanical friction to vessels that already lack cushioning. Forceful massage provides no benefit and may trigger visible bruising. Gentle application techniques, like slow patting, reduce this unnecessary mechanical stress.
Additionally, medical topicals can alter skin resilience. Topical steroids can cause adverse effects such as skin thinning, easy bruising, and increased skin fragility, especially with stronger or prolonged use [DermNet].
Which targeted interventions may protect specific body zones with severe adipose volume loss?
Targeted interventions may protect specific body zones with severe adipose volume loss by matching the protection method to the region’s main weakness: sun exposure, bone proximity, friction, or thin eyelid skin. These interventions focus strictly on dermal atrophy management and external mechanical protection. No topical ingredient can rebuild lost hypodermal fat.
Instead, these strategies aim to enhance remaining tissue resilience. Utilizing padded protective sleeves or sun-protective clothing directly mitigates the environmental stressors that cause rupture. Clinician-guided skincare can further support the epidermal boundary.
Which interventions protect the hands and forearms?
Interventions for the hands and forearms should focus on sun protection, low-friction handling, padded protection during manual tasks, and cautious dermal-support strategies. Utilizing padded sleeves while gardening or cleaning provides a crucial artificial shock absorber. This physical barrier prevents minor bumps from transferring destructive kinetic energy.
Topical support focuses on defending against photodamage. StatPearls states that actinic purpura prevention centers on sun protection and mentions daily sunscreen with SPF greater than 50 for ultraviolet protection [NCBI].
Which interventions protect the shins and lower extremities?
Interventions for the shins and lower extremities should focus on impact reduction, safe footwear and home layout, gentle clothing, and clinician-guided compression when vascular status makes compression appropriate. Clearing walking paths of sharp furniture edges reduces the likelihood of blunt anterior tibial trauma. Wearing long pants or soft shin guards during high-risk activities provides necessary mechanical shielding.
Because fluid dynamics complicate lower-leg healing, any compression strategy must be carefully overseen by a physician. Aggressive massage must be avoided, as it increases shearing force. Any painful, expanding hematoma or skin breakdown on the lower legs demands urgent medical review.
Which interventions protect the periorbital region?
Interventions for the periorbital region should focus on gentle handling, reduced eye rubbing, cautious topical use, and medical review for sudden or unexplained bruising around the eyes. Managing allergies with a clinician reduces the urge to rub this delicate tissue. Applying products with a gentle tapping motion avoids dangerous lateral friction.
Strong active ingredients should be avoided near the eye unless specifically formulated for that area. NCBI Bookshelf describes eyelid skin as having no subcutaneous fat and being the thinnest skin layer of the body, which explains why the periorbital region shows vascular and pigment changes easily [NCBI].
| Body Zone | Primary Cause of Rupture | Topical / Skin-Support Strategy | Physical Protection Strategy |
|---|---|---|---|
| Dorsal hands | UV damage + minor trauma | Sunscreen, cautious retinoids, moisturizer | Gloves or padded sleeves during tasks |
| Extensor forearms | Actinic purpura pattern + shearing force | Photoprotection, dermal support actives | Long sleeves, padded forearm guards |
| Shins / anterior tibia | Bone proximity + impact trauma | Gentle moisturization, skin-tear prevention | Shin guards, home hazard reduction |
| Lower legs | Gravity, edema, vascular factors, impact | Clinician-guided skin care | Clinician-guided compression if appropriate |
| Periorbital region | Thin eyelid skin + rubbing | Eye-safe moisturizers only | Avoid rubbing; treat allergies/irritation |
What daily checklist helps protect high-risk anatomical zones from trauma-induced bruising?
A daily checklist helps protect high-risk anatomical zones from trauma-induced bruising by reducing sun damage, friction, blunt impact, and unsafe rubbing in the exact areas where thinning hypodermal fat leaves vessels exposed. This structured routine focuses on practical trauma prevention across vulnerable body regions. It avoids the misconception that expensive creams can substitute for mechanical protection.
The checklist integrates low-friction handling, physical barriers, and essential clinician review for medication risks. Implementing these daily habits reduces the frequency of visible, trauma-induced bleeding.
How should daily environmental protection reduce regional bruising?
Daily environmental protection should reduce regional bruising by shielding sun-exposed hands and forearms while adding fabric barriers over thin, impact-prone skin. Loose, long sleeves provide a crucial first layer of defense against accidental shearing forces. Padded protective guards offer targeted impact absorption during manual labor or high-risk movement.
Photoprotection stops ongoing ultraviolet extracellular matrix degradation. For actinic purpura prevention, StatPearls mentions daily sunscreen with SPF greater than 50 as part of ultraviolet protection [NCBI].
How should daily physical handling protect fragile skin zones?
Daily physical handling should protect fragile skin zones by replacing rubbing, scrubbing, and forceful application with gentle patting, slow dressing, and low-friction topical application. Drying off with a soft patting motion prevents towel friction from tearing delicate superficial vessels. Similarly, gently smoothing moisturizers onto the shins and forearms avoids dangerous lateral stress.
Avoiding strong adhesive bandages on fragile areas also prevents unnecessary skin tearing upon removal. Practicing this low-friction routine diligently preserves the structural integrity of tissues that lack subcutaneous cushioning.
Daily High-Risk Zone Protection Checklist
FAQs About Areas That Bruise More Easily With Thinning Hypodermal Fat
Which body areas bruise most easily when hypodermal fat thins?
The most vulnerable areas are usually the dorsal hands, extensor forearms, shins, lower legs, and periorbital region. These zones bruise more easily because they have less soft-tissue padding, more friction, more sun exposure, or thinner skin over superficial vessels.
Why do hands and forearms bruise so easily with age?
Hands and forearms bruise easily with age because they combine reduced soft-tissue padding with chronic sun exposure. Senile purpura affects over 10% of people older than 50 years, and lesions commonly occur on extensor forearms and dorsal hands [DermNet].
Why do shin bruises seem larger or slower to heal?
Shin bruises can look larger because the anterior tibia has limited soft-tissue padding over bone. Lower-leg vascular pressure, edema, anticoagulant use, or frail skin can also make bruising more visible or clinically important, especially after minor trauma.
Does under-eye bruising always mean blood vessel rupture?
No. Under-eye darkness can reflect thin eyelid skin, vascular shadowing, pigmentation, edema, or structural hollowing. Sudden bruising around the eye after trauma, vision changes, severe swelling, or unexplained black-eye appearance should be medically evaluated.
Can sunscreen reduce bruising on the arms?
Sunscreen cannot rebuild lost fat, but it can reduce further photodamage that weakens dermal support. StatPearls recommends sun protection for actinic purpura and mentions daily sunscreen with SPF greater than 50 for ultraviolet protection [NCBI].
Can creams rebuild hypodermal fat in high-risk zones?
No topical cream can rebuild lost hypodermal fat in the hands, shins, or under-eye region. Some ingredients may support epidermal or dermal resilience, but physical protection and low-friction handling remain the main practical strategies.
When should regional bruising be checked by a clinician?
Regional bruising should be checked if it is sudden, painful, spreading, unusually large, recurrent without clear trauma, linked to a new medication, or associated with nosebleeds, gum bleeding, blood in urine or stool, fatigue, fever, or weight loss.
Conclusion
Thinning hypodermal fat increases bruising risk most in regions where soft-tissue padding is naturally limited, sun damage is high, friction is frequent, or skin lies close to bone and tendon. The dorsal hands and extensor forearms regularly display actinic purpura because they suffer from both diminished deep fat and chronic photoaging. Meanwhile, the shins and lower legs face frequent blunt impact with very little protective buffering over the tibia.
The periorbital region also highlights this mechanical fragility, as thin eyelid skin easily reveals microtrauma from frequent rubbing. By recognizing these high-risk anatomical zones, patients can implement targeted physical protection, gentle handling, and diligent sun protection instead of relying on ineffective topical cures. It is also vital to undergo a clinician-guided medication review to ensure bleeding risks are safely managed.
At SkinKeeps, we explain skin aging through evidence-based dermatology so readers can understand where their skin is vulnerable and protect it safely. Understanding regional bruising risk helps patients protect fragile skin with location-specific care, calm judgment, and clinical confidence.



