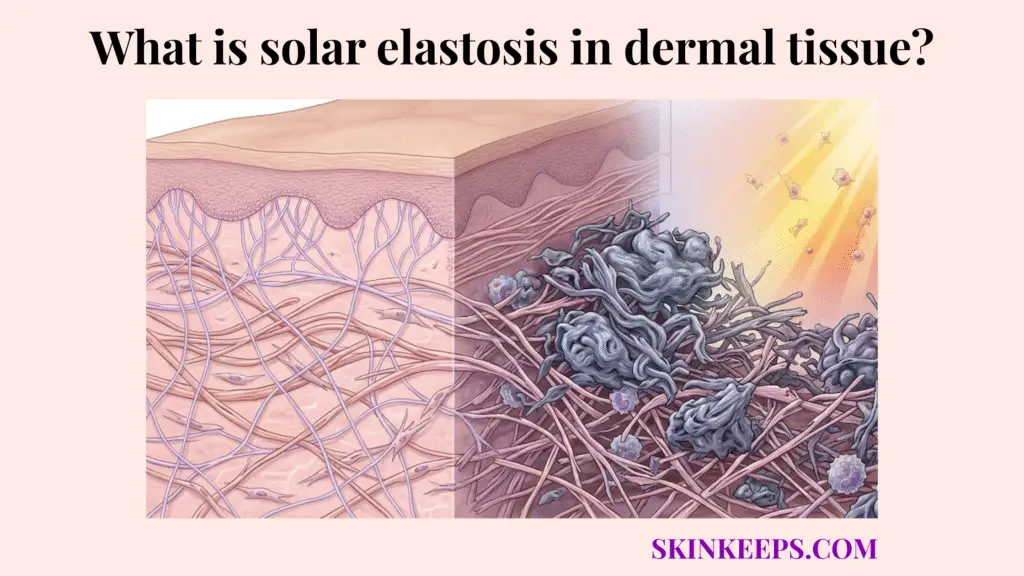
Solar elastosis in dermal tissue is the buildup of abnormal, degraded, non-functional elastic material within the dermis after chronic UV exposure. Instead of preserving a thin, organized elastic network, the skin accumulates thickened, tangled elastotic masses that contribute to leathery texture, yellowing, and deep photoaged wrinkling.
This is fundamentally different from simple age-related thinning or ordinary wrinkle formation. In normal intrinsic aging, structural proteins gently fade away. In severe photoaging, the skin actively overproduces defective material, stuffing the dermis with a chaotic, non-elastic biological sludge that ruins the tissue’s mechanical properties.
Understanding what solar elastosis in dermal tissue is requires examining the clinical baseline, identifying the chronic UV trigger, tracking fibroblast dysfunction, mapping the enzyme imbalance, comparing it to healthy and chronologically aged skin, and applying targeted management.
What is the clinical baseline that defines solar elastosis in dermal tissue?
The clinical baseline that defines solar elastosis in dermal tissue is the accumulation of abnormal elastic material in chronically sun-damaged dermis, not merely a reduction in normal elastin.
Understanding how elastin fibers are arranged in the dermal matrix reveals a delicate, branching network that normally provides resilience. Solar elastosis (also called actinic elastosis) replaces this graceful network with dense, clumped, useless deposits.
Histologically, solar elastosis is described as basophilic degeneration or accumulation of disorganized elastin-containing material in the dermis of photoaged skin. This elastotic material prevents the skin from snapping back, causing the deep furrows frequently seen on the back of the neck or heavily exposed faces of older individuals.
How does chronic UV radiation trigger solar elastosis in dermal tissue?
Chronic UV radiation triggers solar elastosis in dermal tissue by shifting dermal matrix biology toward abnormal elastin-related production and photodamage-associated remodeling, especially under UVA-rich exposure that reaches deeper dermal layers.
This pathology does not develop from a single sunburn. It is the result of relentless, chronic UV exposure penetrating the epidermis and striking the deeper reticular dermis over decades.
Understanding how UV radiation degrades dermal collagen explains why long-standing photoaging literature identifies chronic UV exposure as the main driver of severe elastosis, transforming the skin’s natural repair mechanisms into an uncontrolled, maladaptive cycle.
How does fibroblast dysfunction sustain solar elastosis in dermal tissue?
Fibroblast dysfunction sustains solar elastosis in dermal tissue because chronically UV-damaged fibroblasts stop maintaining normal matrix balance and instead participate in abnormal elastin/tropoelastin production and defective elastic-fiber assembly.
Fibroblasts are the master engineers of the dermal matrix, normally tasked with synthesizing balanced amounts of collagen and tropoelastin (the soluble precursor to elastin). However, severe UV damage severely confuses their programming.
Recent review literature describes solar elastosis as a state in which elastin or tropoelastin synthesis is increased but assembled abnormally because key microfibrillar cofactors are imbalanced. Bernstein et al. (2002) found that ROS exposure caused a greater than sixfold increase in elastin promoter activity, confirming that photoaging can drive abnormal elastin-related overexpression rather than simple decline alone (PubMed, 2002).
How does enzymatic imbalance drive solar elastosis in dermal tissue?
Enzymatic imbalance drives solar elastosis in dermal tissue by degrading healthy elastic architecture while the skin simultaneously produces poor-quality replacement material.
As abnormal tropoelastin floods the tissue, Matrix Metalloproteinases (MMPs) and elastase enzymes attempt to clear the defective debris but ultimately destroy the remaining functional network in the process.
Reviews identify MMP-12, secreted by fibroblasts and macrophages, as an important elastase-like contributor to solar elastosis, and other work implicates cathepsin K in elastic-fiber degradation associated with photoaged skin. This destructive cocktail ensures the dermis is stripped of useful elasticity and filled with biochemical waste.
Elastosis Accumulation Flow
- 1. Chronic UV exposure continues.
- 2. Elastase-like and matrix-degrading enzyme activity rises.
- 3. Healthy elastic structure is degraded.
- 4. Fibroblasts overproduce defective elastic material.
- 5. Abnormal fibers accumulate into dense elastotic masses.
- 6. Skin becomes thickened, yellowed, and less functional.
How does healthy skin compare to the effects of solar elastosis in dermal tissue?
Healthy skin compares very differently to solar elastosis in dermal tissue because normal dermis contains a balanced, functional elastic network, whereas photoaged elastotic dermis contains excessive, abnormal, and mechanically defective elastic material.
Histologic and physical-property studies of photodamaged dermis describe solar elastosis as a major abnormality associated with altered structural behavior. Visually, this translates directly to yellowed leathery skin, contrasting sharply with the translucent, bouncy properties of undamaged tissue.
| Tissue state | Elastin volume | Elastin functionality | Visible texture | Primary cause |
|---|---|---|---|---|
| Healthy dermis | Balanced | Functional and organized | Smooth, resilient, flexible | Normal dermal maintenance |
| Solar elastosis in dermal tissue | Excess abnormal accumulation | Poor, disorganized, non-functional | Thickened, leathery, yellowed, deeply lined | Chronic UV photoaging |
How does chronological aging compare to solar elastosis in dermal tissue?
Chronological aging compares differently to solar elastosis in dermal tissue because intrinsic aging tends to produce a slower, more uniform decline in dermal support, whereas solar elastosis reflects UV-driven abnormal accumulation and disorganization of elastic material. Knowing why collagen density decreases in the dermis with age helps differentiate this gradual thinning from the violent tearing caused by solar radiation.
Reviews of skin aging consistently distinguish intrinsic aging from photoaging on this basis. While chronological aging results in thinner, more fragile, transparent skin, severe photoaging creates a bulky, coarse, and biochemically deranged reticular dermis.
What specific treatments reverse or manage solar elastosis in dermal tissue?
The most useful treatments manage solar elastosis in dermal tissue either by re-regulating dermal matrix behavior or by physically remodeling photodamaged tissue, but advanced solar elastosis is generally managed more realistically than fully reversed.
Recent reviews and clinical studies support prescription retinoids for long-term photodamage improvement and fractional ablative laser resurfacing for structural remodeling in more advanced photoaging.
How do prescription retinoids manage solar elastosis in dermal tissue?
Prescription retinoids manage solar elastosis in dermal tissue by re-signaling skin toward healthier matrix behavior and improving clinical signs of photoaging, but their effects on marked elastotic damage are gradual and incomplete rather than instant or absolute.
Tretinoin fundamentally addresses the fibroblast dysfunction driving the pathology. However, knowing what causes disruption of the epidermal barrier is crucial when using these actives, as inducing chronic surface inflammation can derail deeper dermal recovery. One 1993 histologic study reported that 0.05% tretinoin for 26 weeks had no effect on the degree of solar elastosis, while longer-term follow-up beyond 24 months suggested that elastosis continues to decrease with extended treatment (PubMed, 1993). This confirms that topical intervention is useful, but slow.
How do ablative fractional lasers manage solar elastosis in dermal tissue?
Ablative fractional lasers manage solar elastosis in dermal tissue by physically remodeling photodamaged dermis and stimulating more organized healing in tissue that already contains elastotic damage.
This procedure essentially vaporizes columns of the tangled, elastotic mess, forcing the skin to produce fresh, organized collagen and elastin in its wake. A 2010 study of ablative fractional carbon dioxide laser in photodamaged facial skin found significant clinical improvements and a 40.0% decrease in the subepidermal low-echogenic band (a dermal zone associated with solar elastosis) from 0.078 cm at baseline to 0.038 cm at 3 months (PubMed, 2010).
Management Pathway
- Problem → abnormal elastotic tissue has accumulated in the dermis
- Implication → skin becomes thickened, rigid, and mechanically disorganized
- Solution → regulate fibroblast signaling, reduce further UV injury, and use clinical remodeling procedures when indicated
What are the key summary facts regarding solar elastosis in dermal tissue?
The key summary facts are that solar elastosis in dermal tissue is the accumulation of abnormal, non-functional elastic material after chronic UV exposure, that fibroblast dysfunction and elastase/MMP imbalance help sustain it, and that severe photoaging becomes visibly leathery, yellowed, and deeply lined because the dermal elastic architecture is no longer normal.
Summary Checklist
What steps can you take to treat and prevent solar elastosis in dermal tissue today?
The best practical approach is to treat solar elastosis in dermal tissue as a long-term deep photoaging problem that requires prevention first, then gradual management where needed. Daily UVA-aware sun protection remains the foundation, while retinoids and procedural remodeling are secondary tools for already-damaged skin.
Final Execution Checklist
Quick Answers About Solar Elastosis in Dermal Tissue
What is solar elastosis in dermal tissue?
Solar elastosis in dermal tissue is the buildup of abnormal, disorganized elastin-containing material in chronically sun-damaged dermis. It is a hallmark of advanced photoaging and is different from simple elastin loss or ordinary wrinkling.
Is solar elastosis the same as ordinary wrinkles?
No. Ordinary wrinkling can occur with intrinsic aging, but solar elastosis is a deeper structural pathology in which abnormal elastic material accumulates in the dermis after chronic UV exposure. It produces a thicker, yellower, more leathery form of photoaging.
Why does severe photoaged skin look yellow and leathery?
Because the dermis accumulates disorganized, non-functional elastotic material and undergoes matrix remodeling that changes both texture and structural mechanics. That makes skin less resilient and more coarse, thickened, and deeply lined.
Does UVA play a major role in solar elastosis?
Yes. Long-standing photoaging literature links UVA-rich dermal injury to severe elastosis because UVA reaches deeper connective tissue more effectively than UVB and contributes strongly to fibroblast and matrix stress.
What enzymes are involved in solar elastosis?
Enzymatic imbalance is part of the process. Reviews implicate MMP-12 as an important contributor to solar elastosis development and reduction of functional elastic fibers, and other studies implicate cathepsin K in elastin degradation in photoaged fibroblasts.
Can retinoids treat solar elastosis?
They may help manage it, but gradually. Shorter tretinoin studies showed little direct change in marked solar elastosis over 26 weeks, while longer treatment appears more capable of reducing elastosis over time. That makes retinoids useful but not instant.
Can fractional lasers improve solar elastosis?
Yes, they can help remodel photoaged skin and improve markers linked to elastosis. In one study of ablative fractional CO2 laser, the subepidermal low-echogenic band associated with solar elastosis decreased by 40% at 3 months, alongside broader photoaging improvement.
Is solar elastosis fully reversible?
Not reliably in a complete sense. Management can improve the appearance and remodeling behavior of elastotic skin, but prevention is easier than full reversal, especially once deep structural change is established.
What is the most important prevention step?
Daily UVA-aware broad-spectrum sun protection is the most important prevention step because chronic UV exposure is the core driver of solar elastosis. Other interventions matter more after UV burden is reduced consistently.
Can solar elastosis happen even if skin does not burn much?
Yes. Chronic photoaging damage can accumulate even without dramatic visible burning, especially with repeated UVA-associated dermal exposure. That is one reason solar elastosis is considered a hallmark of long-term photodamage rather than only acute burn injury.
Conclusion
In conclusion, solar elastosis in dermal tissue is a deep structural photoaging pathology in which chronic UV exposure pushes the dermis toward abnormal elastic-material accumulation, enzymatic imbalance, and fibroblast dysfunction rather than healthy elastic maintenance.
That is why advanced photoaged skin becomes thickened, leathery, yellowed, and less functional over time. Management can improve this state, but the strongest strategy remains early and consistent UVA-aware prevention.