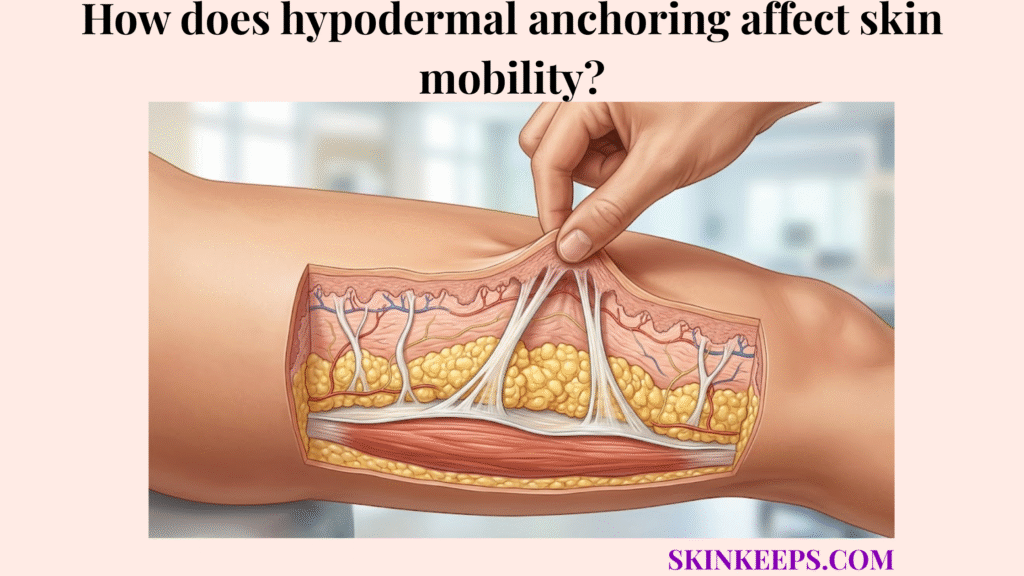
Hypodermal anchoring affects skin mobility by keeping the skin attached to deeper structures while allowing controlled glide over muscles, tendons, joints, and fascia. This delicate balance ensures the body can move freely without tearing the superficial layers or losing mechanical support.
This guide explores how subdermal tethering manages friction, shear force, and viscoelasticity to maintain healthy skin movement. We examine what happens when adhesions restrict motion or laxity causes excessive looseness, while outlining realistic clinical modalities and daily fascial mobility support.
Why is healthy subdermal tethering essential for normal biomechanical movement?
Healthy subdermal tethering is essential for normal biomechanical movement because the skin must remain supported while still sliding over muscles, tendons, joints, and fascia during motion. If the skin were rigidly fixed in place, everyday actions would cause severe restriction and discomfort. The hypodermis supports adipose storage, insulation, and structural anchoring to safely manage these competing physical demands.
This unique architectural design allows the body to stretch dynamically while preserving a strong, interconnected foundation.
How does skin glide support movement over tendons and muscles?
Skin glide supports movement over tendons and muscles by allowing the dermis and subcutaneous layer to shift slightly while remaining mechanically connected to deeper structures. This controlled sliding prevents the superficial layers from being traumatized during muscular contraction or joint flexion.
Consequently, healthy tissue glide ensures smooth, pain-free range of motion across the entire body.
How does the hypodermis dissipate friction and shear force?
The hypodermis dissipates friction and shear force by using soft adipose lobules and fibrous septae to absorb, redirect, and distribute movement-related stress. External friction acting on the skin surface is absorbed by this underlying buffer layer before it reaches the deep muscle.
As a result, this network ensures that deeper tissues experience far less concentrated stress during physical impact.
How do subcutaneous retaining ligaments permit multidirectional skin mobility?
Subcutaneous retaining ligaments permit multidirectional skin mobility by anchoring the dermis to deeper fascia through flexible connective bands that stretch, recoil, and guide controlled movement. Because fibrous septa connect layers in the hypodermis, these structures act as a dynamic scaffolding system.
Their oblique or variable orientation allows the skin to move smoothly in multiple directions without fully detaching.
How does the elastic septal network guide skin movement?
The elastic septal network guides skin movement by combining collagen-based tensile support with elastin-related recoil inside the subcutaneous anchoring system. Collagen provides the sturdy framework that prevents overstretching, while elastin permits the bands to return toward their resting length after movement.
This coordinated stretch and release ensures the skin returns smoothly to its original position after active motion.
How does the viscoelasticity of fat lobules support glide?
The viscoelasticity of fat lobules supports glide because adipose compartments can deform under pressure and then help the tissue return toward its resting shape. These soft, deformable compartments sit between the fibrous bands, preventing direct friction between rigid tissue layers.
This unique composition allows the subcutaneous tissue to absorb compressive loads effortlessly without disrupting the gliding plane.
| Component | Material | Biomechanical Function | Role in Skin Glide |
|---|---|---|---|
| Fibrous septae | Collagen-rich connective tissue | Tensile support and anchoring | Guides controlled movement |
| Elastin fibers | Elastic protein network | Recoil after stretch | Supports return toward resting shape |
| Fat lobules | Deformable adipose compartments | Cushioning and displacement | Reduces concentrated friction |
| Superficial fascia | Connective fascial plane | Layer organization | Coordinates deeper glide |
| Dermis | Collagen-elastin skin layer | Surface resilience | Translates deeper movement to surface |
| Extracellular matrix | Structural protein network | Tissue integrity | Maintains mobility environment |
What happens to fascial attachments when scars and fibrosis restrict natural skin mobility?
Fascial attachments can restrict natural skin mobility when scars, adhesions, or fibrosis make connective tissue less extensible and reduce normal glide between skin and deeper layers. When the healing process lays down disorganized collagen, the resulting scar tissue often binds normally separate layers together.
This abnormal binding creates a highly restricted range of motion across the affected area.
How do tissue adhesions and sclerosis limit skin glide?
Tissue adhesions and sclerosis limit skin glide by creating stiffer connective areas that resist normal sliding between the dermis, hypodermis, and superficial fascia. These fibrotic connections act like internal anchor points that physically block the tissues from shifting laterally.
Consequently, the affected skin may feel tight and functionally compromised during movement.
How can restricted mobility create puckering or tightness?
Restricted skin mobility can create puckering or tightness when tethered tissue pulls the skin inward or limits how far the skin can stretch during movement. As the surrounding healthy tissue attempts to glide, the rigid scar adhesion acts as a fixed point, causing the surface to dimple or retract.
Clinician-guided evaluation is highly recommended if painful or function-limiting scars develop.
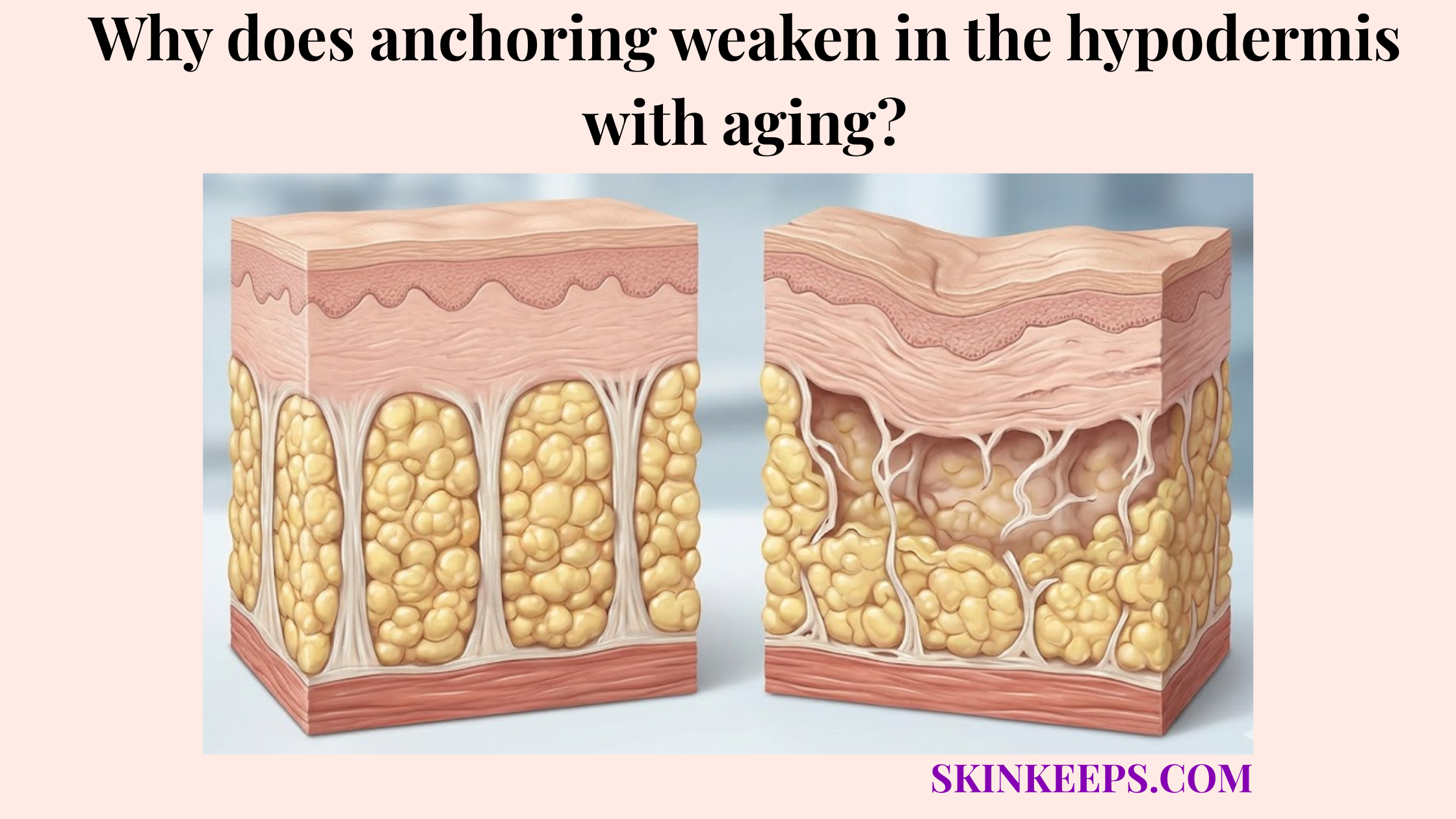
Why does degradation of deep connective anchors cause excessive skin mobility and laxity?
Degradation of deep connective anchors can cause excessive skin mobility and laxity when collagen and elastin support weaken enough to reduce recoil, tension, and controlled positioning. When anchoring weakens in the hypodermis with aging, the fascial network loses its ability to hold the skin firmly against the deeper planes.
This lack of structural tension presents outwardly as visible looseness.
How do elastin depletion and plastic deformation affect skin recoil?
Elastin depletion and plastic deformation affect skin recoil by reducing the ability of connective anchors to stretch and return toward their original length after repeated loading. Once these bands stretch beyond their natural recovery limit, they become permanently elongated.
This biological wear and tear ensures that collagen density decreases in the dermis with age, compounding the structural failure.
How does gravitational shear contribute to sagging?
Gravitational shear can contribute to sagging when weakened anchors allow the skin and subcutaneous tissue to shift downward more easily under long-term mechanical load. As the fascial attachments loosen, they can no longer resist the constant, downward pull of gravity.
This chronic mechanical stress ultimately results in visible tissue descent and shifting contours.
| Mobility Problem | Biomechanical Cause | Common Appearance | Functional Meaning |
|---|---|---|---|
| Adhesion / restriction | Excess tethering or stiff scar tissue | Puckering, tight scar, limited skin glide | Movement may feel restricted |
| Fibrosis / sclerosis | Denser connective tissue | Firmness, tethered texture | Tissue may be less extensible |
| Laxity | Reduced collagen/elastin tension | Loose or mobile skin | Tissue may sag or shift |
| Plastic deformation | Stretch beyond elastic recovery | Persistent looseness | Recoil may be reduced |
| Balanced mobility | Flexible anchoring + soft tissue glide | Smooth movement | Skin remains supported and mobile |
What myths should be avoided about stretching or tightening hypodermal skin attachments?
Myths should be avoided about stretching or tightening hypodermal skin attachments because these connective structures respond differently from muscles, surface skin, or temporary tightening products. Many cosmetic claims mistakenly suggest that extreme physical manipulation or surface lotions can dictate deep fascial tension.
Believing these misconceptions often leads to inappropriate tissue handling or unmet clinical expectations.
Why can aggressive stretching worsen already lax skin attachments?
Aggressive stretching can worsen already lax skin attachments because excessive pulling may increase mechanical strain on connective tissue that has already lost some recoil. Forcefully stretching loose skin does not trigger it to snap back tightly.
Instead, this excessive manipulation may irritate or further overstress an already compromised fascial network.
Why do surface firming products not restore deep mechanical glide?
Surface firming products do not restore deep mechanical glide because temporary epidermal tightening does not remodel the deeper anchoring network that controls subcutaneous movement. While these products may temporarily improve surface hydration or texture, they do not release internal adhesions.
True mechanical glide requires structural flexibility across the deep fascial planes.
Which clinical modalities may restore healthier tension to compromised hypodermal anchor points?
Clinical modalities may restore healthier tension to compromised hypodermal anchor points by either releasing restrictive tethering, improving scar mobility, or stimulating collagen remodeling in lax support layers. Because energy-based devices tighten dermal tissue, they provide an option for laxity, while manual or surgical release addresses restrictions.
Selecting the right intervention depends entirely on whether the tissue is too tight or too loose.
How can subcision or scar-focused therapy release restrictive tethering?
Subcision or scar-focused therapy may release restrictive tethering by mechanically separating selected fibrotic bands or mobilizing stiff scar tissue under clinician supervision. For certain cellulite-like depressions or tethered scars, this controlled release minimizes the rigid downward pull.
Physical therapy or manual mobilization may also support this process by gently improving restricted range of motion.
How can microfocused ultrasound and radiofrequency support lax anchors?
Microfocused ultrasound and radiofrequency may support lax anchors by delivering controlled thermal energy that can stimulate collagen remodeling in selected skin and subcutaneous support layers. MFU-V devices can deliver treatment at focal depths such as 1.5 mm, 3.0 mm, and 4.5 mm, which supports its use as a layer-targeted energy treatment for selected laxity concerns. [JCAD]
| Pathology | Biomechanical Cause | Treatment Goal | Clinical Intervention Category |
|---|---|---|---|
| Too tight / adhesion | Excess tethering or scar stiffness | Improve glide and extensibility | Scar therapy, subcision, clinician-guided mobilization |
| Too stiff / fibrosis | Dense connective tissue | Reduce tethered texture | Subcision or selected device-based therapy |
| Too loose / laxity | Reduced collagen-elastin tension | Support collagen remodeling | MFU-V, radiofrequency, biostimulation |
| Surface dryness only | Epidermal barrier issue | Improve texture/hydration | Topicals and barrier care |
| Functional limitation | Pain or reduced range of motion | Restore movement safely | Medical evaluation or physical therapy |
What daily checklist helps preserve healthy biomechanical glide of the fascial network?
A daily checklist helps preserve healthy biomechanical glide of the fascial network by combining comfortable movement, gentle tissue mobility, collagen support, hydration, and avoidance of harsh mechanical stress. Daily support routines prioritize maintaining the current elasticity and preventing unnecessary strain.
These practical habits act as long-term maintenance rather than instant cures.
How can manual mobilization habits support tissue glide?
Manual mobilization habits can support tissue glide when they use gentle, tolerable pressure to keep skin and subcutaneous tissue moving comfortably over deeper layers. Light massage or skin rolling may help maintain baseline tissue comfort without causing bruising or pain.
However, any painful, restricted, or post-surgical scars should always be evaluated professionally.
How can hydration and nutritional support protect anchor elasticity?
Hydration and nutritional support can protect anchor elasticity by supporting normal extracellular matrix function, collagen maintenance, and tissue comfort. Ensuring adequate protein, vitamin C, zinc, and copper intake provides the biological building blocks required for natural collagen turnover.
Furthermore, adequate daily hydration supports the fluid balance necessary for optimal viscoelasticity.
Daily Fascial Glide & Anchor Preservation Checklist
FAQs About Hypodermal Anchoring and Skin Mobility
What does skin glide mean?
Skin glide means the skin and subcutaneous layer can move slightly over deeper muscles, tendons, joints, and fascia while staying mechanically supported. Healthy glide allows movement without excessive pulling, stiffness, or uncontrolled looseness.
How does the hypodermis help skin move?
The hypodermis helps skin move by combining soft fat lobules with fibrous septae and fascia-based support. This structure allows controlled sliding, friction distribution, shock absorption, and mechanical connection between the dermis and deeper tissue planes.
Can scars restrict skin mobility?
Yes. Scar tissue, adhesions, or fibrosis may restrict skin mobility when connective tissue becomes less extensible or more tethered to deeper layers. Painful, tight, or function-limiting scars should be assessed by a qualified clinician or physical therapist.
Why does aging make skin feel looser?
Aging can make skin feel looser because collagen, elastin, fat support, and retaining structures gradually change. These changes can reduce recoil and controlled tension, allowing the skin and subcutaneous tissue to shift more visibly under gravity.
Can massage restore skin glide?
Massage may support comfort and tissue mobility in some cases, but it should not be presented as guaranteed adhesion release or deep-anchor repair. Painful scars, surgical tethering, or restricted range of motion should be handled with clinician-guided care.
Which treatments target tight or loose anchors?
Tight anchors may require scar therapy, physical therapy, or selected release procedures. Loose anchors may be addressed with energy-based collagen remodeling such as MFU-V or radiofrequency. [JCAD]
Can daily habits preserve hypodermal mobility?
Daily habits may support hypodermal mobility by maintaining comfortable movement, avoiding harsh mechanical stress, supporting collagen maintenance, and protecting skin from UV damage. These habits support tissue health but do not guarantee correction of scars or laxity.
Conclusion
Hypodermal anchoring affects skin mobility by balancing attachment and glide through fibrous septae, fat lobules, fascia, collagen, and elastin. When the system is too tight, skin may feel tethered; when it is too loose, laxity and tissue descent may become more visible.
At SkinKeeps, we explain skin structure through evidence-based dermatology and anatomy. Understanding skin mobility helps readers separate realistic fascial support from exaggerated tightening or release claims.