
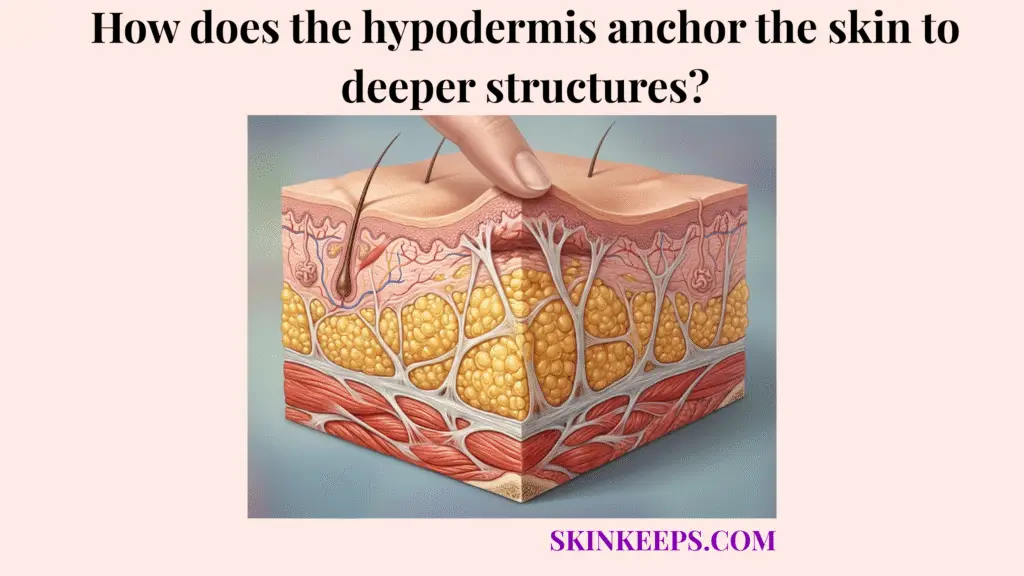
The hypodermis anchors the skin to deeper structures through collagen- and elastin-rich connective tissue bands that link the dermis, subcutaneous fat, superficial fascia, and deeper fascial planes. This mechanical connection prevents the skin envelope from shifting unpredictably over the underlying anatomy.
This guide covers how retinacula cutis influence skin mobility and shock absorption, while exploring the biological factors contributing to aging-related laxity. We also separate tightening myths from reality, evaluating clinical treatments and daily support strategies that aim to maintain fascial integrity safely.
What exactly are the retinacula cutis and how do they form the skin’s deep anchoring system?
Retinacula cutis form the skin’s deep anchoring system by creating fibrous connections that pass through subcutaneous fat and link the dermis with deeper fascial support layers. By securing these levels together, fibrous septa connect layers in the hypodermis to prevent severe structural detachment.
This fundamental hypodermal anchoring architecture explains why the skin stays firmly attached to the body contour despite constant daily motion.
How do retinacula cutis organize the hypodermal anchoring network?
Retinacula cutis organize the hypodermal anchoring network by running through the subcutaneous fat layer as collagen-rich fibrous septae that support fat compartments and connect skin to deeper fascia. These bands essentially tuft the subcutaneous tissue, binding the upper skin envelope through the fat down to the deep fascial floor.
This structural grid ensures mechanical support and maintains an even distribution of adipose lobules.
How does the superficial fascia interface support skin anchoring?
The superficial fascia interface supports skin anchoring by providing a connective tissue plane where hypodermal septae, fat compartments, and deeper fascial structures interact. In facial anatomy, specialized layers like the superficial musculoaponeurotic system (SMAS) help tether the skin tightly to underlying muscle groups.
This dermal-fascial connection ensures coordinated movement across highly expressive zones without localized structural failure.
Why is flexible subcutaneous tethering crucial for muscle movement and shock absorption?
Flexible subcutaneous tethering is crucial for muscle movement and shock absorption because the skin must stay mechanically connected to deeper structures while still gliding over moving muscles and joints. Because hypodermal anchoring affects skin mobility, these structures must stretch and recoil smoothly.
If tissue lacked this controlled flexibility, every joint movement would forcefully shear the skin away from its underlying blood supply.
How does tissue glide support normal movement?
Tissue glide supports normal movement by allowing the skin and subcutaneous layer to shift slightly over deeper muscles without losing structural support. This dynamic gliding plane prevents traumatic tension buildup during high-impact actions like running or bending.
Connective tissue elasticity ensures the skin returns safely to its resting position once the movement ceases.
How do hypodermal anchors dissipate mechanical force?
Hypodermal anchors dissipate mechanical force by combining soft fat compartments with elastic fibrous bands that spread blunt pressure across a wider tissue area. During an impact, the compressible fat absorbs the initial blow, while the tensile bands quickly distribute the kinetic energy.
This mechanical force dissipation prevents concentrated mechanical stress from easily rupturing local blood vessels or tearing deep tissue.
| Anatomical Requirement | Role of Fat | Role of Fibrous Bands | Biomechanical Result |
|---|---|---|---|
| Skin attachment | Adds volume and padding | Links dermis to fascia | Skin remains supported |
| Movement | Allows soft displacement | Controls excessive sliding | Skin glides without losing support |
| Shock absorption | Compresses under pressure | Spreads tension through septae | Force is distributed |
| Shape stability | Maintains contour | Resists downward drift | Tissue position is preserved |
| Aging response | May reduce or redistribute | May stiffen or stretch | Laxity becomes more visible |
How does degradation of fascial connective tissue lead to visible skin sagging?
Degradation of fascial connective tissue can lead to visible skin sagging when collagen, elastin, and retaining structures lose enough strength or elasticity to resist gravity and repetitive mechanical stress. When anchoring weakens in the hypodermis with aging, the structural integrity of the entire skin envelope inevitably declines.
This progressive failure reveals itself outwardly as noticeable tissue laxity and altered body contours.
How does loss of elasticity affect retaining ligaments?
Loss of elasticity affects retaining ligaments by reducing their ability to maintain tension and recoil after repeated stretching, facial movement, or gravitational loading. In the face, elongated retaining ligaments may contribute to visible jowling or downward fat pad descent over decades.
Once stretched beyond their natural recovery limit, these bands cannot automatically return to their original, taut position.
How is ligamentous laxity different from fat loss?
Ligamentous laxity is different from fat loss because laxity describes weakened support tension, while fat loss describes reduced volume within the supported tissue compartment. Aging typically involves both processes simultaneously, complicating the visible structural decline.
While volume replacement may camouflage mild changes, it does not physically shorten a stretched deep anchoring matrix.
Which biological and mechanical stressors accelerate failure of hypodermal attachments?
Biological and mechanical stressors may accelerate failure of hypodermal attachments by stretching collagen networks, stiffening connective tissue, or reducing the elastic recoil that helps anchors recover after load. Chronic environmental strain forces the fascial connective tissue to endure tension it cannot successfully repair.
Over time, these daily cumulative insults may exceed the tissue’s natural elastic recovery limits.
How can rapid weight fluctuation stress hypodermal anchors?
Rapid weight fluctuation can stress hypodermal anchors because tissue expansion and contraction repeatedly load the fibrous septae that help hold the skin envelope to deeper structures. Severe, cyclic volume changes push the connective bands into plastic deformation, meaning they remain permanently lengthened.
Consequently, gradual and sustainable weight management represents a much safer approach for preserving long-term structural support.
How can advanced glycation end-products stiffen anchoring collagen?
Advanced glycation end-products can stiffen anchoring collagen by increasing cross-linking in structural proteins, which may reduce flexibility and resilience in connective tissue over time. This process of glycation transforms normally pliable fibers into rigid, brittle structures that easily fracture under tension.
Reducing factors that promote excessive glycation may gently support the maintenance of a flexible subcutaneous tethering system.
What myths should be avoided about tightening loose subdermal ligaments without surgery?
Myths should be avoided about tightening loose subdermal ligaments without surgery because deep anchoring structures cannot be physically shortened or lifted by surface-level products alone. The cosmetic market regularly exaggerates the capabilities of topical formulations to combat fundamental structural laxity.
Setting realistic expectations prevents frustration and redirects focus toward treatments that actually influence deep mechanical support.
Why can’t lifting creams shrink elongated hypodermal retaining ligaments?
Lifting creams cannot shrink elongated hypodermal retaining ligaments because topical products primarily act at the skin surface and cannot mechanically contract deep fascial attachments. While hydrating ingredients may temporarily improve surface smoothness, they do not possess the capacity to physically reconstruct the skin-fascia linkage.
Understanding this limitation ensures patients do not rely on lotions for true structural repair.
Why doesn’t facial exercise shorten stretched anchoring bands?
Facial exercise does not shorten stretched anchoring bands because muscle contraction and connective tissue anchoring are different biological systems. While exercising may alter facial muscle tone or expression fullness, it does not reverse the micro-tears and laxity present in deep subdermal ligaments.
Therefore, relying on repetitive movement to fix structural sagging lacks a solid biomechanical foundation.
Which clinical procedures may remodel or support the skin-to-muscle structural bond?
Clinical procedures may remodel or support the skin-to-muscle structural bond by heating, contracting, or stimulating connective tissue layers involved in dermal and subcutaneous support. Because energy-based devices tighten dermal tissue, these clinician-guided treatments can sometimes provoke a mild lifting response.
However, actual results vary substantially based on individual connective tissue health and specific anatomical severity.
How can microfocused ultrasound and radiofrequency target deeper support layers?
Microfocused ultrasound and radiofrequency can target deeper support layers by delivering controlled energy that heats selected tissue zones and may stimulate collagen remodeling. MFU-V devices can target tissue depths such as 1.5 mm, 3.0 mm, and 4.5 mm, allowing treatment energy to reach from superficial dermis toward deeper support layers in selected protocols. [JCAD]
How can biostimulators support connective tissue remodeling?
Biostimulators may support connective tissue remodeling by stimulating collagen production in selected dermal or subdermal planes, depending on product, dilution, placement, and patient selection. Injectables like hyperdilute calcium hydroxylapatite or poly-L-lactic acid aim to gradually reinforce the tissue matrix rather than mechanically pulling it upward.
These methods may improve laxity and texture over time, serving as a biological support strategy.
| Procedure | Target Layer | Mechanism of Action | Degree of Lift Language |
|---|---|---|---|
| Microfocused ultrasound | Dermis, subdermis, selected deeper support layers | Focused thermal coagulation points | May improve laxity in selected patients |
| Radiofrequency | Dermis and subcutaneous support depending on device | Heat-based collagen remodeling | May improve firmness or texture |
| Hyperdilute CaHA | Dermal/subdermal connective tissue planes | Collagen-stimulating biostimulation | Supports skin quality, not ligament shortening |
| PLLA | Dermal/subdermal tissue | Gradual collagen stimulation | May improve laxity and texture over time |
| Surgical lifting | SMAS/fascial support layers | Tissue repositioning and fixation | Most direct for true tissue repositioning |
| Topical creams | Epidermis/superficial dermis | Hydration and surface support | Cannot mechanically shorten deep anchors |
What daily checklist helps preserve elasticity of the deep fascial network?
A daily checklist helps preserve elasticity of the deep fascial network by reducing avoidable mechanical stress, supporting collagen maintenance, and protecting connective tissue from lifestyle factors that may accelerate stiffness. Consistent implementation of these low-risk habits fosters a supportive environment for the body’s natural fascial network preservation.
While not a cure for established laxity, proactive care minimizes preventable structural degradation.
How can weight and tension management protect hypodermal attachments?
Weight and tension management can protect hypodermal attachments by reducing repeated expansion, contraction, and mechanical shear across the subcutaneous connective tissue network. Avoiding rapid weight cycling spares the fascial connective tissue from excessive, irreversible stretching.
During high-impact activities, using supportive garments may improve comfort and help reduce aggressive tissue bounce.
How can biochemical preservation support connective tissue elasticity?
Biochemical preservation can support connective tissue elasticity by protecting collagen and elastin from avoidable degradation while providing nutrients needed for normal tissue repair. Ensuring adequate protein, vitamin C, and zinc intake supplies the necessary building blocks for ongoing matrix renewal.
Furthermore, applying daily sunscreen defends against UV radiation, preserving the overarching dermal support above these deep attachments.
Daily Hypodermal Anchor Preservation Checklist
FAQs About Hypodermal Anchoring to Deeper Structures
What anchors the skin to deeper structures?
Retinacula cutis and fibrous septae help anchor the skin by connecting the dermis, subcutaneous fat, and fascia. These connective tissue bands organize fat compartments, provide support, and allow controlled movement between skin and deeper tissues.
Is the hypodermis only a fat layer?
No. The hypodermis contains fat, blood vessels, nerves, connective tissue septae, and anchoring structures. Its role is not only energy storage; it also supports skin mobility, shock absorption, insulation, and mechanical attachment to deeper planes.
How does the SMAS relate to skin anchoring?
The SMAS is a facial fibromuscular support layer involved in facial soft-tissue organization. It is region-specific and should not be treated as identical across the body. In facial anatomy, it helps explain how superficial tissues relate to deeper support layers.
Do creams tighten deep hypodermal anchors?
No topical cream can mechanically shorten deep hypodermal anchors or retaining ligaments. Creams may improve hydration, surface smoothness, or superficial skin quality, but deep fascial support usually requires energy-based, injectable, or surgical approaches when treatment is appropriate.
Can facial exercise re-anchor sagging skin?
Facial exercise may change muscle activity or facial expression patterns, but it does not directly shorten stretched retaining ligaments. Skin laxity involves dermis, fat, fascia, ligaments, bone support, and connective tissue quality, not muscle tone alone.
Which non-surgical treatments target deeper support layers?
Microfocused ultrasound and radiofrequency are commonly discussed for deeper support-layer remodeling. MFU-V protocols may use treatment depths such as 1.5 mm, 3.0 mm, and 4.5 mm, depending on device and indication. [JCAD]
Can daily habits preserve hypodermal anchoring?
Daily habits cannot permanently rebuild deep anchors, but they may support connective tissue resilience. Gradual weight changes, sun protection, regular movement, adequate nutrition, and avoiding harsh mechanical stress can help preserve the tissue environment around hypodermal attachments.
Conclusion
The hypodermis anchors the skin to deeper structures through retinacula cutis, fibrous septae, superficial fascia, and region-specific fascial support systems. These structures allow the skin to stay supported while still gliding, cushioning force, and adapting to movement.
At SkinKeeps, we explain skin structure through evidence-based dermatology and anatomy. Understanding hypodermal anchoring helps readers separate realistic connective tissue support from exaggerated tightening claims.



