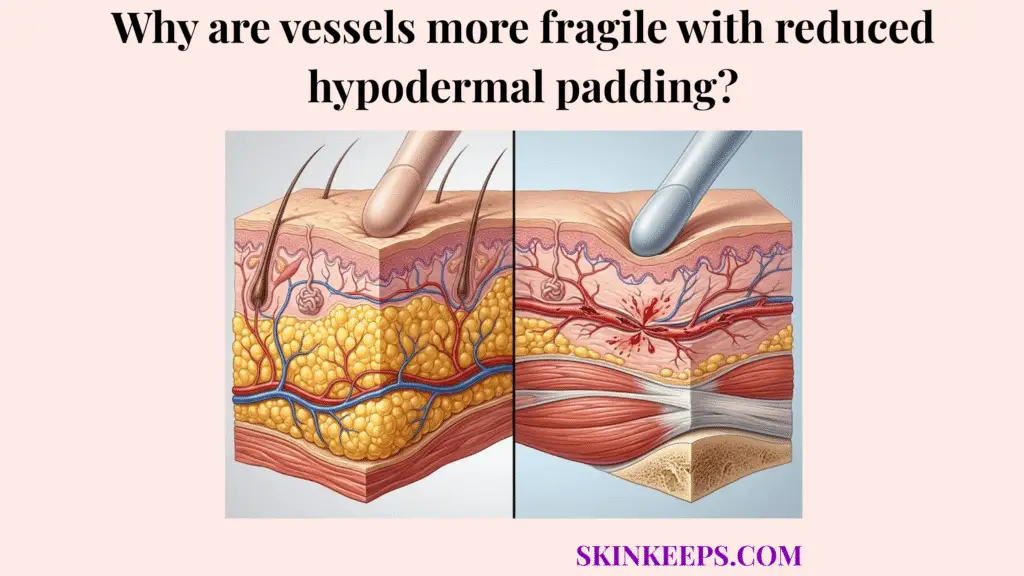
Blood vessels become more fragile with reduced hypodermal padding because the skin loses part of the soft subcutaneous tissue support that normally cushions, stabilizes, and protects superficial blood vessels from minor trauma. This support loss transfers external mechanical stress directly into the fragile capillary walls.
This guide explains how padding loss causes mechanical vascular fragility, how extracellular matrix breakdown worsens the issue, and why daily physical protection is necessary. It also covers how to recognize structural actinic purpura and when unusual bruising requires a clinical review.
What is the anatomical relationship between deep fat cushioning and blood vessel stability?
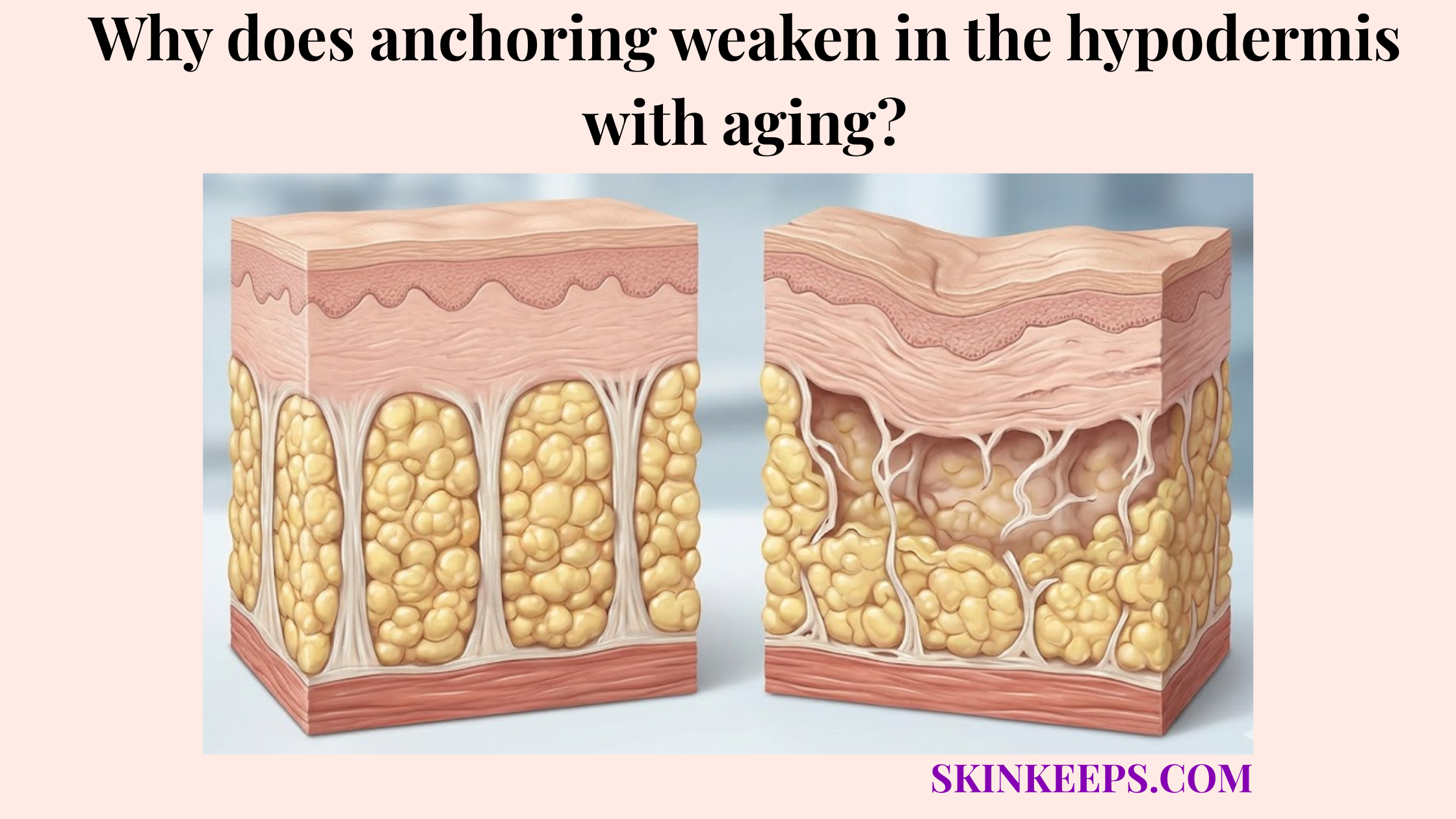
The anatomical relationship between deep fat cushioning and blood vessel stability is that hypodermal adipose tissue supports the skin’s vascular network by cushioning movement, spreading force, and reducing direct stress on superficial blood vessels. This deep fat layer provides the necessary structural foundation for the entire cutaneous circulation system.
Hypodermal adipose tissue consists of specialized fat-storing lobules anchored beneath the dermis. These adipose lobules actively buffer the vascular network against sudden tissue movement or compression. By anchoring these structures securely, the padding reduces the risk of vascular tearing.
How does the adipose matrix act as a structural anchor for blood vessels?
The adipose matrix acts as a structural anchor for blood vessels by surrounding them with fat lobules and fibrous septae that reduce twisting, compression, and traction during ordinary skin movement. These sturdy connective partitions organize the white adipose tissue into supportive compartments. This compartmentalization prevents excessive structural tension on delicate vascular walls.
In addition to the deep fat, dermal collagen and elastin also help secure these superficial vessels in place. When this combined tissue support fails, age-related fragility becomes highly visible. Consequently, senile purpura affects over 10% of people aged over 50 years [DermNet].
How does hypodermal cushioning absorb kinetic energy before vessels rupture?
Hypodermal cushioning absorbs kinetic energy before vessel rupture occurs by compressing under pressure and distributing impact force across a wider tissue area instead of concentrating force directly on capillary walls. Kinetic energy from a bump or blunt impact naturally travels through the soft tissue. Thicker padding dissipates this energy harmlessly.
When the padding is thin, more force transfers directly into the vascular structures. This concentrated pressure causes immediate blood leakage into the surrounding skin. Fortunately, these structural actinic purpura lesions typically resolve within 1 week to 3 weeks [NCBI].
Why does reduced hypodermal padding directly cause mechanical vascular fragility?
Reduced hypodermal padding directly causes mechanical vascular fragility because superficial blood vessels lose part of the soft tissue support that normally protects them from compression, friction, and shearing force. Without this buffer, external physical forces are transmitted straight into the fragile vascular architecture.
Compression occurs when direct pressure flattens the skin against deeper structures. Friction happens when surfaces rub repeatedly against the epidermis. Both actions increase visible bruising risk when the subcutaneous cushioning loss leaves the vessels exposed.
Shearing involves a lateral pulling motion across the skin layers. This lateral stress tears the capillary walls when trauma transfer is no longer mitigated by underlying fat.
What happens when the protective padding effect is lost?
When the protective padding effect is lost, superficial blood vessels become more exposed to pressure from the skin surface and less insulated from harder underlying structures such as fascia, muscle, or bone. This dual exposure traps the fragile vessels between the external impact and the rigid internal anatomy.
Bumping a forearm on a table easily demonstrates this vulnerability. The thin skin compresses immediately against the bone, causing rapid vascular trauma. This is why the dorsal hands and extensor forearms are such common visible sites for bruising.
Why does shearing force tear unsupported capillary walls more easily?
Shearing force tears unsupported capillary walls more easily because thin skin can slide or pull across deeper tissue without enough cushioning to absorb the lateral stress. This friction-related bruising often happens from tight clothing, scrubbing, or aggressive massage.
The mechanical cascade follows a predictable pattern in vulnerable tissue:
- Pressure compresses vessels.
- Friction pulls tissue laterally.
- Reduced padding transfers both forces to fragile vessels.
When these vessels tear, they create distinct patterns of bleeding. Petechiae are small purpuric lesions up to 2 mm, while ecchymoses are larger extravasations of blood [DermNet].
| Tissue State | Padding Level | Resistance to Shearing Force | Rupture Risk |
|---|---|---|---|
| Well-supported skin | Higher subcutaneous cushioning | Force spreads across a wider tissue area | Lower visible bruising risk |
| Photoaged thin skin | Reduced dermal and hypodermal support | Vessels receive more direct stress | Higher purpura risk |
| Medication-amplified bruising | Support may be weakened or clotting altered | Microbleeds may appear larger | Bruises may persist visually |
| High-friction exposure | Padding cannot absorb lateral pull | Capillaries tolerate more shear | Bruising or skin tears become more likely |
How does connective tissue breakdown worsen unsupported capillary weakness?
Connective tissue breakdown worsens unsupported capillary weakness because collagen and elastin normally reinforce the skin matrix around vessels, and their degradation removes a second layer of mechanical support. This vascular support matrix resides primarily within the dermis and the extracellular matrix.
The extracellular matrix provides essential structural integrity. When this matrix weakens, dermal atrophy follows, leaving the capillary network completely unanchored.
- Collagen fibers provide the rigid tensile support that prevents vessels from over-expanding.
- Elastin fibers supply the recoil support that helps tissue snap back safely after stretching.
- The combined loss of both proteins causes severe structural support failure around the vessel walls.
How does extracellular matrix degradation weaken vessel support?
Extracellular matrix degradation weakens vessel support by reducing the collagen and elastin framework that normally stabilizes superficial blood vessels within the dermis and upper subcutaneous tissue. The extracellular matrix consists of these vital structural proteins that hold the vascular architecture together.
When these proteins break down, the surrounding tissue loses its density and firmness. This structural decline means vessels leak more easily after minor trauma. Actinic purpura lesions typically resolve within 1 week to 3 weeks [NCBI].
Why does reduced vascular rebound capacity increase bruising?
Reduced vascular rebound capacity increases bruising because vessels in a weakened matrix have less elastic support to stretch, recover, and tolerate repeated pressure without leaking blood. Healthy elastin provides the recoil necessary for tissues to deform safely and return to their original shape.
Without this elasticity, mechanical stress physically tears the rigid vessel walls. This creates visible blood leakage into the skin, typically appearing as purple macules or ecchymoses. Highlighting this common mechanical failure, senile purpura prevalence is approximately 10% in elderly individuals [PMC].
Which medications and external stressors accelerate rupture risk in exposed superficial vessels?
Medications and external stressors accelerate rupture risk in exposed superficial vessels by either weakening skin structure, increasing visible bleeding after microtrauma, or degrading the collagen matrix that supports fragile vessels. Systemic or potent topical corticosteroids are strongly associated with skin thinning and dermal atrophy.
This corticosteroid-induced dermal atrophy removes the remaining connective tissue support. In contrast, anticoagulants and antiplatelet drugs act as clotting modifiers rather than tissue-thinning agents. They alter the clotting response, which can worsen medication-amplified bruising after an injury occurs.
How do anticoagulants and corticosteroids worsen visible bruising?
Anticoagulants and corticosteroids worsen visible bruising through different mechanisms: anticoagulants affect clotting after a vessel leaks, while corticosteroids can contribute to skin thinning, purpura, and fragility. Corticosteroids weaken the architectural support around the vessels by inducing dermal atrophy.
Anticoagulants and antiplatelet drugs, such as warfarin, aspirin, clopidogrel, and NSAIDs, make bruises more noticeable or persistent after a small vessel injury. They do not make the vessels structurally fragile, but they increase the volume of blood that escapes.
Any medication review to address these side effects must be clinician-guided. Patients should never stop prescribed blood thinners without professional medical instruction.
How does UV radiation damage vascular support?
UV radiation damages vascular support by driving chronic photodamage, dermal atrophy, collagen degradation, and loss of tissue reinforcement around superficial blood vessels. Chronic photodamage is the long-term structural harm caused by persistent ultraviolet exposure.
This UV exposure weakens the entire vascular support matrix, not just the vessel wall itself. The dorsal hands and extensor forearms are especially vulnerable to this damage, requiring only minor trauma to cause visible bleeding. Emphasizing this link, senile purpura affects over 10% of people older than 50 years, and chronic sunlight exposure is listed as a risk factor [DermNet].
What myths should be avoided when treating trauma-prone blood vessels?
Treatment myths should be avoided when treating trauma-prone blood vessels because many common assumptions confuse structural vessel fragility with simple vitamin deficiency, poor circulation, or a surface hydration problem. Believing these wrong treatment assumptions can misdirect care and delay practical prevention.
For instance, a common myth is that surface hydration repairs mechanical support loss. While moisturizers improve epidermal dryness, they do not replace deep subcutaneous padding.
Another myth assumes all easy bruising stems from poor circulation or bleeding disorders. While unexplained bruising requires a safety warning and medical evaluation, localized actinic purpura is often a structural issue.
Why is the “Vitamin C cure-all” idea misleading for trauma-prone vessels?
The vitamin C cure-all idea is misleading for trauma-prone vessels because age-related actinic purpura is usually driven by structural tissue fragility, not automatically by systemic deficiency. Severe vitamin C deficiency can cause bleeding problems, but that requires a specific medical diagnosis.
Topical or oral vitamin C may support collagen biology as an antioxidant. However, megadosing this nutrient does not rebuild lost hypodermal padding.
If persistent, unexplained bruising occurs, a clinician evaluation is necessary. This ensures proper diagnosis, given that senile purpura affects over 10% of people older than 50 years [DermNet].
Why can aggressive massage and scrubbing worsen fragile vessels?
Aggressive massage and scrubbing can worsen fragile vessels because they increase friction and shearing force on skin that already lacks adequate hypodermal cushioning. Friction occurs when surfaces rub repeatedly, while shearing force creates a lateral pull across the tissue layers.
Stimulating blood flow vigorously is not always safe for fragile skin. Patients should adopt low-friction care, opting to gently pat the skin dry instead of rubbing it with a towel.
Avoiding harsh scrubs, adhesive trauma, and tight clothing prevents unnecessary tearing. Actinic purpura lesions often remain visible for 1 week to 3 weeks, so one friction event may leave visible discoloration for weeks [NCBI].
Which topical treatments and clinical interventions may help reinforce fragile vascular structures?
Topical treatments and clinical interventions may help reinforce fragile vascular structures by supporting the surrounding dermal matrix, reducing further photodamage, and improving trauma protection, but they cannot rebuild lost hypodermal padding. Care generally focuses on matrix-supporting strategies, adjunctive bruise-care ingredients, and physical protection.
It is important to avoid promising total vessel repair from skincare alone. While certain active ingredients may improve visible support, external mechanical protection remains the most direct prevention strategy for trauma-prone skin.
How can retinoids support surrounding dermal thickening?
Retinoids may support surrounding dermal thickening by encouraging collagen formation in photodamaged skin, which can improve the structural envelope above fragile vessels over time. Retinoids are vitamin A–derived compounds that support long-term dermal remodeling.
They primarily support dermal collagen density rather than restoring hypodermal fat. For example, treatment with tretinoin produced an 80% increase in collagen I formation, compared with a 14% decrease with vehicle, in a photodamaged skin study [PubMed].
Retinoids should be used cautiously on fragile elderly skin due to irritation risks. Their application should be clinician-guided to prevent further skin barrier damage.
What role do vitamin K, rutin, tranexamic acid, and other vasoprotective ingredients play?
Vitamin K, rutin, tranexamic acid, and other vasoprotective ingredients should be framed as adjunctive support options, not as proven methods for rebuilding vessel walls or replacing lost hypodermal padding. Vitamin K is sometimes used cautiously in skincare to assist with bruise appearance.
Rutin functions as a bioflavonoid, while topical tranexamic acid targets pigment and bleeding-related pathways. Clinical evidence for these ingredients varies significantly by formulation and skin condition.
None of these topical agents can restore deep anatomical padding. The topical vitamin K laser-bruising study assessed bruising on days 0, 3, 7, 10, 14, and 17, finding only lower severity scores post-treatment, not absolute prevention [PubMed].
| Intervention | Mechanism | Strengthens Matrix or Vessel? | Clinical Efficacy Language |
|---|---|---|---|
| Retinoids | Support collagen formation in photodamaged skin | Mainly matrix support | Evidence-supported for photoaged collagen biology, not a direct bruise cure |
| Vitamin C | Collagen cofactor and antioxidant support | Matrix support | Supportive, not a cure-all |
| Vitamin K | May affect bruising appearance in some post-procedure contexts | Bruise-care adjunct | Mixed/limited evidence; do not overclaim |
| Rutin | Bioflavonoid with capillary-support rationale | Adjunctive vessel support | Condition-specific evidence; avoid broad claims |
| Tranexamic acid | Used in dermatology mainly for pigment/bleeding-related pathways | Adjunctive | Do not claim actinic purpura repair without direct evidence |
| Protective clothing | Reduces friction and impact | External mechanical protection | Most direct prevention strategy for trauma-prone skin |
| Medication review | Identifies exacerbating drugs | Risk management | Must be clinician-guided |
What daily checklist helps protect compromised blood vessels from mechanical tearing?
A daily checklist helps protect compromised blood vessels from mechanical tearing by reducing friction, limiting impact, preventing additional photodamage, and ensuring medication-related bruising risk is reviewed safely. Practical trauma prevention provides the most direct benefit for thin skin.
The checklist integrates clinician review, gentle skin care, and UV protection. It focuses on external mechanical protection rather than product-specific routines.
How should environmental and physical protection be used daily?
Environmental and physical protection should be used daily by treating fragile skin with low-friction care, reducing blunt impacts, and covering vulnerable areas during activities that commonly cause forearm trauma. Patients should pat dry with towels and avoid tight, constrictive sleeves that create friction.
Wearing soft long sleeves or padded guards during gardening, cleaning, or carrying groceries offers direct mechanical prevention. Actinic purpura lesions may remain visible for 1 week to 3 weeks, so preventing trauma is often more practical than trying to clear bruises after they form [NCBI].
How should long-term vascular health be managed?
Long-term vascular health should be managed through consistent photoprotection, gentle skin care, and clinician-guided review of medications that may worsen bruising visibility or skin fragility. Consistent use of sunscreen and sun-protective clothing helps limit structural connective tissue breakdown.
Patients should seek a medication review if bruising and skin thinning are worsening, but they must never stop blood thinners independently. A red-flag evaluation is necessary for unexplained or widespread bleeding. Senile purpura affects over 10% of people older than 50 years, making long-term protection relevant for many aging-skin readers [DermNet].
Daily Vascular Protection Checklist
FAQs About Reduced Hypodermal Padding and Fragile Blood Vessels
Does reduced hypodermal padding make blood vessels break more easily?
Yes. Reduced hypodermal padding makes superficial blood vessels easier to injure because the skin loses part of the soft support that absorbs pressure and friction. This support loss transfers more mechanical stress into fragile vessels after minor trauma.
Is fragile blood vessel bruising the same as a blood disease?
Not always. Fragile blood vessel bruising in older, sun-damaged skin is often structural and benign. However, sudden, widespread, painful, or unexplained bruising can signal medication effects or a bleeding disorder and should be checked by a healthcare professional.
Why do fragile-vessel bruises appear mostly on the hands and forearms?
Fragile-vessel bruises often appear on the dorsal hands and extensor forearms because these areas receive chronic sun exposure and have less soft-tissue padding. This location pattern fits the common presentation of actinic purpura.
How long do actinic purpura bruises usually last?
Actinic purpura lesions commonly resolve within 1 week to 3 weeks, although visible discoloration may concern patients while it fades. This timeline supports prevention-focused care because avoiding trauma is often easier than clearing bruises after they form [NCBI].
Do blood thinners make vessels fragile?
Blood thinners do not usually make vessels structurally fragile. They affect clotting after a vessel leaks, which can make bruises larger, darker, or more persistent. Any medication concern should be reviewed with the prescribing clinician.
Can vitamin C stop fragile-vessel bruising?
Vitamin C supports collagen biology, but it should not be presented as a cure for trauma-induced bruising from reduced hypodermal padding. If vitamin deficiency is suspected, diagnosis and treatment should be guided by a healthcare professional.
Can topical creams rebuild lost hypodermal padding?
No topical cream can rebuild lost hypodermal padding. Some ingredients may support the epidermis or dermal matrix, but reduced subcutaneous cushioning requires practical protection strategies such as reducing friction, using protective clothing, and preventing further photodamage.
Clinical Key Takeaway
Actinic purpura on the hands and forearms is predominantly a structural issue driven by severe hypodermal depletion and cumulative photodamage. While topical supports may incrementally enhance remaining dermal resilience, the most effective management strategy depends mainly on consistent physical protection—acting as an external shock absorber—and routine medical evaluation of exacerbating medications.
Conclusion
Reduced hypodermal padding makes blood vessels more fragile because the loss of connective tissue support allows ordinary pressure, friction, and shearing force to reach superficial blood vessels more directly. Without adequate deep tissue buffering, the skin loses its natural mechanical protection against daily trauma.
Managing this mechanical fragility requires combining physical protection with a cautious clinical review of exacerbating stressors like UV exposure and medications. At SkinKeeps, we explain skin aging through evidence-based dermatology so readers can understand the mechanics behind visible skin changes and protect fragile skin safely.
Understanding vessel fragility as a mechanical support problem helps patients protect their skin with clarity, caution, and confidence.