
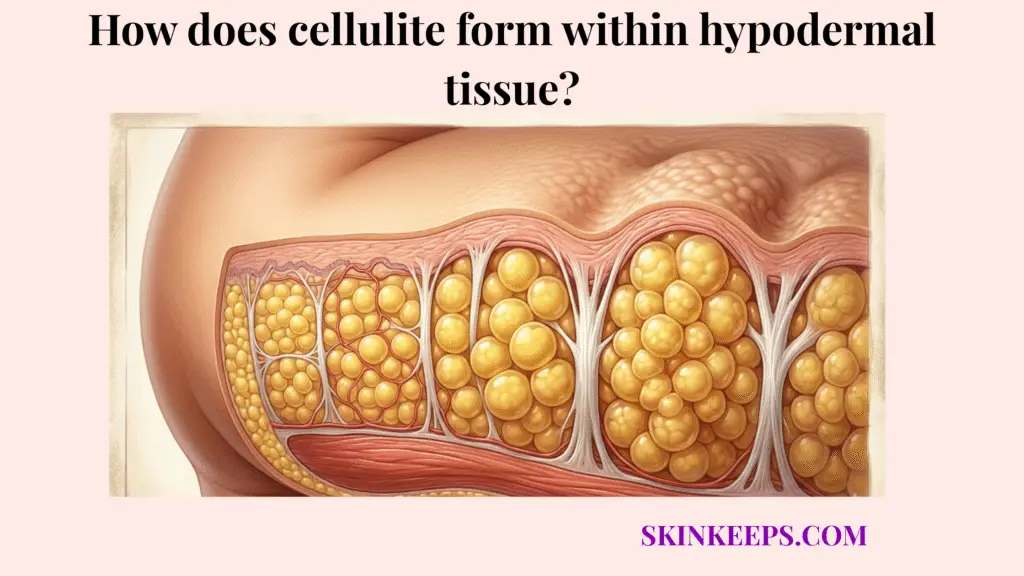
Cellulite forms within hypodermal tissue when fat lobules push upward toward the dermis while fibrous connective tissue bands pull downward, creating uneven surface tension. This mechanical push-and-pull creates a dimpled skin appearance, marking a structural pattern rather than a simple accumulation of excess fat.
The underlying hypodermis relies on adipocytes and fibrous septae to create the deeper support structure of the skin. This guide explains how that specific tissue architecture drives cellulite formation, why treatments must target anatomical changes, and how to manage skin appearance safely.
What exactly is the biological mechanism of cellulite formation in the hypodermis?
The biological mechanism of cellulite formation in the hypodermis is a structural distortion where enlarged or upward-shifting fat lobules press against the dermis while fibrous septae tether parts of the skin downward. This uneven distribution of pressure disrupts the normally smooth subcutaneous tissue layer.
These fat lobules are simply clusters of adipocytes grouped into distinct compartments by surrounding connective tissue. When these fat-storing cells enlarge or lose even support, they actively push upward against the dermis and alter the external skin contour.
Simultaneously, the collagen-rich fibrous septae that divide these lobules act as anchors connecting deeper tissue to the overlying skin. When these anchoring bands and expanding fat cells fall out of mechanical balance, the skin surface reflects the internal distortion as visible dimpling.
How does the dermal-fat interface shape cellulite formation?
The dermal-fat interface shapes cellulite formation because this boundary between the dermis and the subcutaneous fat layer must remain smooth for the skin surface to look even. Cellulite directly disrupts that critical boundary through simultaneous upward fat pressure and downward connective tissue tethering.
This structural unevenness makes the dimpling highly visible across affected skin areas. Consequently, cellulite affects approximately 80% to 90% of postpubertal women, marking it as a common physiological texture pattern rather than a rare disorder [PubMed].
How does the push-and-pull mechanic create cellulite dimples?
The push-and-pull mechanic creates cellulite dimples because fat lobules push upward against the dermis while fibrous septae pull selected points of the skin downward. This opposing mechanical force creates an uneven surface tension across the affected skin areas.
That uneven tension appears externally as characteristic mattress-like depressions or dimpling. Because this mechanism is deeply structural, simple surface-level changes cannot effectively correct it without addressing the underlying mechanical tension.
Why do fibrous connective tissue bands cause the characteristic dimpling of hypodermal fat?
Fibrous connective tissue bands cause the characteristic dimpling of hypodermal fat because they tether the skin downward while surrounding fat compartments bulge upward around those fixed points. These bands act as rigid anchors connecting the skin surface to deeper muscle fascia.
When the surrounding fat lobules expand, the fixed bands refuse to stretch, pulling the skin down to create a dimple. This structural tethering acts as the primary driver of deep depressions across the skin surface.
Treatments that do not address this connective tissue tension generally yield minimal structural improvement. Identifying this tethering effect ensures patients seek realistic interventions.
How does septal stiffening increase cellulite dimpling?
Septal stiffening increases cellulite dimpling because less flexible fibrous septae pull downward more persistently, preventing the skin from stretching smoothly over the fat layer. This stiffness is often driven by fibrosis, which gradually thickens and hardens the connective tissue over time.
Additionally, glycation processes form Advanced Glycation End-products (AGEs) that bind to proteins and further exacerbate this collagen stiffness. These rigid bands exert a much stronger downward tethering force on the dermal-fat interface.
Clinicians often use the Nürnberger–Müller scale to categorize how this progressive stiffness and fat protrusion worsen cellulite severity from grade 0 to grade 3.
How does adipocyte herniation push hypodermal fat upward?
Adipocyte herniation pushes hypodermal fat upward when enlarged or poorly supported fat lobules protrude toward the dermis instead of remaining evenly contained within their connective tissue compartments. When these adipocytes expand, the entire fat compartment swells and presses aggressively against the overlying skin boundary.
This upward pressure creates the raised areas of skin located directly between the tethered dimples. This structural pattern is exceptionally common in female tissue, as cellulite affects 80% to 90% of women after puberty, while less than 10% of men experience it [Cleveland Clinic].
| Component | Normal Function | Cellulite Dysfunction | Visible Result |
|---|---|---|---|
| Fat lobules | Provide soft hypodermal volume | Bulge upward unevenly | Raised areas around dimples |
| Fibrous septae | Divide fat compartments and tether tissue | Pull selected skin points downward | Depressions or dimples |
| Dermis | Provides smooth surface support | Loses firmness or elasticity | Uneven texture becomes more visible |
| Extracellular matrix | Supports collagen and elastin structure | May become stiff or weakened | Reduced tissue flexibility |
| Microcirculation | Supports tissue oxygenation and fluid balance | May contribute to swelling or tissue congestion | Cellulite may look more pronounced |
How do hormonal and sex-related tissue differences influence structural tethering within the subcutaneous layer?
Hormonal and sex-related tissue differences influence structural tethering within the subcutaneous layer by affecting fat distribution, connective tissue architecture, and how easily fat lobules protrude toward the skin surface. These inherent anatomical differences dictate how the skin responds to underlying adipose expansion.
Female tissue patterns inherently predispose the dermal-fat interface to uneven tension. Because men and women have different septal structures, expanding fat causes different visible surface reactions.
Recognizing this biological reality helps patients understand that cellulite is an anatomical pattern rather than a lifestyle failure. It prevents the shame often incorrectly associated with cellulite visibility.
How may estrogen-related changes affect microcirculation and connective tissue?
Estrogen-related changes may affect cellulite visibility by influencing estrogen-related fat distribution, microcirculation, connective tissue behavior, and fluid balance within the hypodermal layer. As a primary sex hormone, estrogen helps direct where the body stores fat and indirectly influences microcirculation through small vessels in the skin.
When local blood flow slows, researchers propose that mild hypoxia may contribute to subtle inflammation and subsequent septal fibrosis. When these fluid balances shift, the surrounding dimpled appearance can look more pronounced.
Why is cellulite more common in female tissue architecture?
Cellulite is more common in female tissue architecture because the arrangement of fibrous septae and subcutaneous fat compartments can allow upward fat protrusion to become more visible at the skin surface. In many women, these connective tissue bands run vertically, creating straight downward tethers.
In men, the septal network typically forms a crisscrossed pattern that contains fat more evenly. Because of these vertical bands, upward fat pressure easily creates distinct, visible depressions.
Consequently, this structural difference explains why cellulite affects approximately 80% to 90% of postpubertal women but remains rare in men [PubMed].
Why is localized adipose herniation biologically different from ordinary weight gain?
Localized adipose herniation is biologically different from ordinary weight gain because cellulite depends on tissue architecture, septal tethering, and dermal support, not only on the total amount of body fat. This process of subcutaneous tissue herniation creates upward bulging that is firmly anchored by stiff connective bands, which do not simply disappear with caloric restriction.
While general weight gain increases fat volume globally, localized adipose herniation relies on specific mechanical tension beneath the skin. This explains why athletic individuals with low body fat can still display visible dimpling.
Recognizing this biological difference prevents unrealistic expectations regarding diet and exercise.
How does volume differ from architecture in cellulite formation?
Fat volume differs from architecture in cellulite formation because fat-cell size can change with body weight, while fibrous septae and dermal support determine whether the skin surface becomes tethered and uneven. Losing weight reduces the overall size of the fat lobules pressing against the skin.
However, reducing fat volume does not stretch or release the stiff connective tissue bands tethering the dermis downward. This structural reality means that while weight loss may reduce visible dimpling slightly, it may not fully resolve the uneven surface tension.
Which metabolic and lifestyle factors may worsen degradation of the dermal-fat interface?
Metabolic factors and lifestyle factors may worsen degradation of the dermal-fat interface by affecting collagen quality, fluid balance, circulation, inflammation, and the septal stiffness of connective tissue. These external and systemic influences do not single-handedly create cellulite, but they can exacerbate existing structural weaknesses.
Poor fluid dynamics or damaged collagen makes underlying fat protrusion more obvious. When the surrounding dermal matrix loses its firm, elastic resilience, the fat lobules face less resistance.
Consequently, minimizing these worsening factors forms the foundation of any non-invasive management plan.
How may sedentary behavior and lymphatic stagnation affect cellulite appearance?
Sedentary behavior may affect cellulite appearance by reducing muscle-driven circulation and lymphatic movement, which can make fluid retention and tissue congestion more visible in cellulite-prone regions. Because lymphatic drainage relies heavily on daily muscle contraction, prolonged inactivity severely reduces the natural movement of fluid through lymphatic vessels.
When movement is minimal, interstitial fluid accumulates in the subcutaneous tissue. This temporary fluid retention swells the tissue around the tethered septae, making the dimples appear deeper.
Regular walking and resistance training support this fluid balance, subtly improving overall skin texture.
How can glycation affect collagen-rich septae?
Glycation can affect collagen-rich septae by making collagen fibers stiffer over time, which may reduce connective tissue flexibility and increase visible tethering. The extracellular matrix provides a vital collagen and elastin network that supports both the skin and its underlying fat compartments.
Collagen gives this matrix tensile strength, while elastin helps the tissue stretch and recoil. Additionally, glycation processes form Advanced Glycation End-products (AGEs) that bind to proteins and further exacerbate this collagen stiffness.
This stiffness increases the downward pull on the skin surface, actively worsening the structural dimpling effect over time.
What treatment myths should be avoided when addressing fibrotic hypodermal bands?
Treatment myths should be avoided when addressing fibrotic hypodermal bands because cellulite is a deep structural pattern, and surface-level products cannot permanently release tethered fibrous septae. The skincare market frequently promotes unverified solutions promising flawless skin by targeting supposed toxins.
These claims completely ignore the biological reality of downward tethering and upward fat protrusion. Relying on these topical myths delays practical, realistic management of the skin’s appearance.
Understanding that deep structural architecture requires clinician-guided evaluation is essential for setting healthy expectations.
Why can’t caffeine creams break fibrous cellulite tethers?
Caffeine creams cannot break fibrous cellulite tethers because topical products may temporarily affect skin texture or fluid appearance, but they do not physically release deep connective tissue bands. Topical products like caffeine cream may temporarily tighten or dehydrate the skin surface to create a smoother look.
While they may reduce superficial swelling, they are biologically incapable of cutting or remodeling rigid collagen bands. Patients may enjoy the short-lived surface improvements, but they should treat these creams as daily maintenance rather than permanent structural correctors.
AAD explains that while creams may produce temporary appearance changes, medical procedures are required to target tough bands beneath the skin [AAD].
Why can vigorous scrubbing or dry brushing fail to correct deep cellulite architecture?
Vigorous scrubbing or dry brushing fails to correct deep cellulite architecture because surface friction cannot remodel the fibrous septae and fat compartments that sit deeper within the hypodermis. Dry brushing may temporarily increase local circulation and cause mild surface swelling that temporarily masks small dimples.
However, scraping the epidermis does not alter the underlying extracellular matrix or release stiff connective tissue. Aggressive friction can also irritate sensitive skin without offering any structural benefit.
Patients should handle their skin gently, understanding that mechanical scrubbing cannot undo localized adipose herniation.
Which clinical procedures physically target architectural distortion of the deep fat layer?
Clinical procedures may physically target architectural distortion of the deep fat layer by releasing tethered fibrous septae, remodeling dermal collagen, or reducing focal fat bulging, depending on the procedure. These medical interventions actively bypass the epidermis to alter the structural mechanics of the hypodermis.
Different devices apply distinct mechanisms to either cut stiff bands or apply energy to the surrounding matrix. Because these procedures physically alter tissue, they must be clinician-guided and require careful patient selection.
While they may improve appearance, they carry potential side effects like bruising, swelling, or pain.
How does subcision release cellulite-causing septae?
Subcision releases cellulite-causing septae by mechanically cutting selected fibrous bands that pull the skin downward, allowing the depressed surface to lift more evenly. This minimally invasive procedure directly targets the rigid tethering structures responsible for creating the deepest surface dimples.
By releasing these specific anchors, the upward fat pressure is allowed to smooth out against the dermis. This targeted release directly addresses the core mechanical failure of cellulite.
The AAD reports that in a 232-patient study evaluating tissue-stabilized guided subcision, 99% of patients were satisfied, with results lasting 2 years or longer [AAD].
How do acoustic wave, radiofrequency, and laser treatments differ?
Acoustic wave therapy, radiofrequency, and laser treatment differ because they use different forms of energy to improve cellulite appearance through tissue stimulation, heating, collagen remodeling, or fat-septae targeting. Acoustic wave therapy utilizes mechanical pressure waves to stimulate tissue, whereas radiofrequency relies on thermal energy to heat the tissue and support collagen remodeling.
Laser treatment uses targeted light energy to heat or remodel dermal collagen and fat structures simultaneously. These energy devices aim to improve the resilience of the extracellular matrix over time.
For example, a recent acoustic subcision study reported significant short-term improvement at 12 weeks, demonstrating that energy treatments support appearance improvement rather than permanent removal [PMC].
| Procedure | Main Target | Mechanism of Action | Clinical Longevity Language |
|---|---|---|---|
| Subcision | Fibrous septae | Releases tethered bands beneath dimples | Can provide longer-lasting improvement in selected patients |
| Tissue-stabilized guided subcision | Septae | Uses controlled release of bands | Evidence includes multi-year follow-up in studies |
| Acoustic wave therapy | Tissue stiffness / circulation | Mechanical wave stimulation | May improve appearance short-term; maintenance may be needed |
| Radiofrequency | Dermis and fat layer | Heat-based collagen remodeling | Improvement may be modest and temporary |
| Laser treatment | Fat, septae, dermis | Energy-based remodeling | Results depend on device and treatment plan |
| Topical products | Skin surface | Hydration or temporary texture change | Cannot release deep septae |
What daily checklist helps manage structural progression of subcutaneous tissue herniation?
A daily checklist helps manage structural progression of subcutaneous tissue herniation by supporting circulation, collagen maintenance, muscle tone, and low-irritation skin care without claiming to erase cellulite. Realistic daily management focuses on optimizing the biological environment surrounding the fat lobules and fibrous septae.
Small supportive habits can subtly improve tissue flexibility and visible skin texture over time. This proactive routine empowers patients to maintain healthy hypodermal architecture safely.
Avoiding aggressive, painful treatments ensures the dermal-fat interface remains resilient rather than inflamed.
How can daily movement support circulation and lymphatic flow?
Daily movement can support circulation and lymphatic flow by using muscle contraction to move blood and fluid through tissues that otherwise remain compressed or sedentary for long periods. Regular walking, taking standing breaks, and incorporating resistance training act as natural pumps for the lymphatic system.
This active fluid movement prevents localized congestion around the fat lobules. While exercise will not snap fibrous bands, it optimizes the tissue environment and improves underlying muscle tone.
This healthy muscle base provides a firmer foundation for the overlying hypodermal tissue.
How can structural nutrition support collagen turnover?
Structural nutrition can support collagen turnover by providing amino acids, vitamin C, and overall dietary adequacy needed for normal connective tissue maintenance. The extracellular matrix relies on a steady supply of nutrients to repair daily wear and prevent excessive stiffening.
Maintaining adequate protein intake supports the structural integrity of the dermal envelope above the fat layer. This supportive approach builds resilience without promoting restrictive diets that cause unnecessary stress.
Consistent, balanced nutrition helps the body naturally maintain its complex connective tissue network.
Daily Hypodermal Architecture & Circulation Checklist
FAQs About Cellulite Formation in Hypodermal Tissue
Is cellulite just excess fat?
No. Cellulite is not just excess fat. It forms when fat lobules, fibrous septae, and the dermal-fat interface create uneven mechanical tension beneath the skin. Fat volume can influence visibility, but tissue architecture drives the dimpled pattern.
How common is cellulite?
Cellulite is very common. Evidence reviews describe cellulite as present in approximately 80–90% of postpubertal women, which supports framing it as a common physiological skin texture pattern rather than a rare disease [PubMed].
Why is cellulite more common in women?
Cellulite is more common in women because sex-related tissue architecture, fat distribution, hormones, and skin thickness can make upward fat protrusion and downward septal tethering more visible. Cleveland Clinic reports 80–90% of women after puberty have cellulite, compared with less than 10% of men [Cleveland Clinic].
Can weight loss remove cellulite?
Weight loss may reduce fat volume and make cellulite less visible for some people, but it does not necessarily release fibrous septae or correct structural tethering. This is why cellulite can still appear in people with lower body fat.
Can caffeine creams remove cellulite?
Caffeine creams may temporarily improve surface texture by affecting hydration or firmness, but they cannot physically release deep fibrous septae. Medical procedures that target connective bands work through different mechanisms than topical products.
Which procedure targets cellulite bands most directly?
Subcision targets cellulite bands most directly because it mechanically releases selected fibrous septae beneath tethered dimples. AAD reports that in a 232-patient study of Cellfina, 99% of patients were satisfied, with results lasting 2 years or possibly longer [AAD].
Can daily habits cure cellulite?
Daily habits cannot cure cellulite, but movement, gentle skin care, sun protection, and adequate nutrition may support tissue health and reduce factors that make dimpling look more pronounced. The goal is realistic management, not permanent removal.
Conclusion
Cellulite forms within hypodermal tissue when fat lobules, fibrous septae, and dermal support create uneven mechanical tension that appears as dimpling on the skin surface. This visible texture change is a common consequence of sex-related tissue architecture and normal adipocyte herniation. While topical creams provide only temporary aesthetic changes, clinician-guided procedures can mechanically target the underlying connective tissue tethering.
At SkinKeeps, we explain skin structure through evidence-based dermatology so readers can understand visible skin changes without shame, exaggeration, or false treatment promises. Understanding cellulite as a structural hypodermal pattern helps readers choose realistic care with clarity, caution, and confidence.



