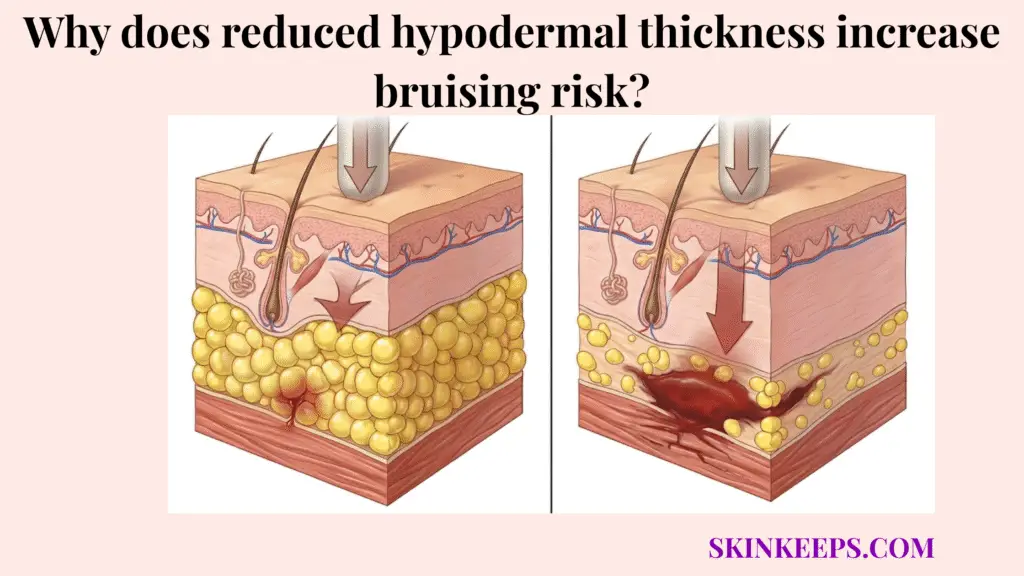
Reduced hypodermal thickness increases bruising risk because the skin loses part of its deep adipose cushioning system. Fragile superficial blood vessels become less protected from minor daily impacts, friction, and pressure.
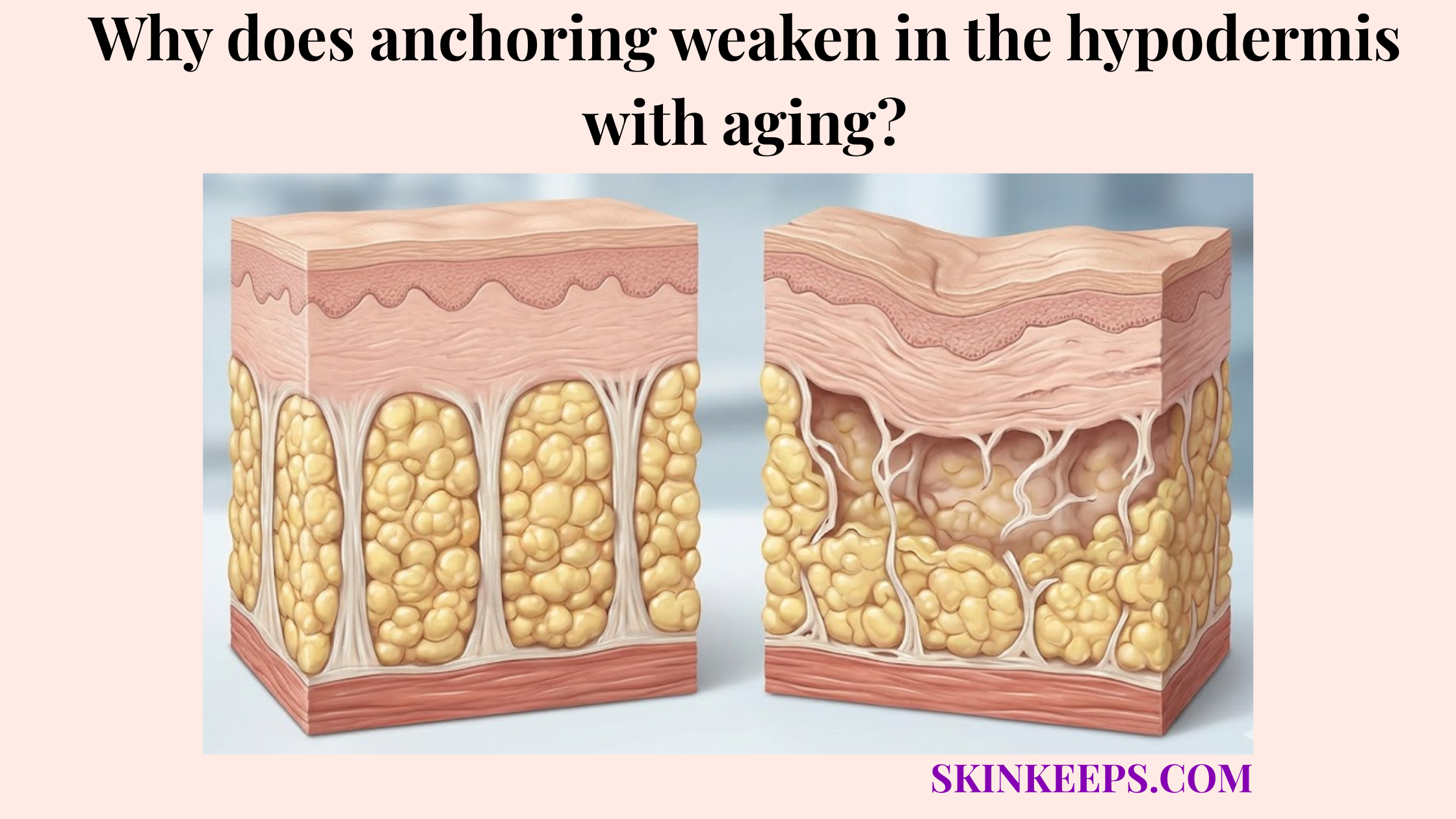
The hypodermis is the subcutaneous layer beneath the dermis. It contains adipocytes, adipose lobules, and fibrous septae that help cushion and anchor the skin. This guide explains how that padding loss causes bruising, how to recognize actinic purpura, and when easy bruising should be checked by a clinician.
What is the mechanical relationship between reduced hypodermal thickness and skin trauma?
The mechanical relationship between reduced hypodermal thickness and skin trauma is direct: a thinner subcutaneous fat layer absorbs less impact force. Minor bumps, pressure, and friction can therefore transfer more stress into the dermis and its superficial blood vessels.
The hypodermis cushions the skin through adipose lobules supported by fibrous septae. As this essential hypodermal fat decreases with age, the skin loses part of its physical buffer against everyday trauma.
A histologic study of donor sites found the radial forearm hypodermis measured roughly 1,913 ± 1,066 µm. This makes the radial forearm one of the naturally thinner sampled donor-site regions (Hwang et al., 2016) [PubMed].
A healthy hypodermis acts like thick protective padding. When that padding wears thin, the fragile surface bears greater mechanical stress from minor impacts.
How does the hypodermis act as a biological shock absorber?
The hypodermis acts as a biological shock absorber by using adipocyte-rich lobules and fibrous septae to spread mechanical force across a wider tissue area. Adipocytes are specialized fat-storing cells filled with compressible lipids. They momentarily deform under pressure to gracefully absorb kinetic energy.
However, loose fat cells require structural architecture to work properly. Fibrous septae organize these fat cells into distinct lobules and anchor the skin. This support mechanism diffuses surface pressure, reducing direct mechanical stress on superficial dermal vessels.
Why are the forearms and hands more vulnerable when skin becomes thin?
The forearms and hands become more vulnerable when skin becomes thin because these sun-exposed areas often have less soft-tissue padding and more cumulative photodamage. Even in youth, the backs of the hands and the extensor forearms lack deep fat reserves.
As collagen density decreases with age, these regions lose essential dermal and subcutaneous support. Minor pressure can then produce visible purple patches. Clinical authorities consistently identify these areas as the primary sites for actinic purpura (DermNetNZ, 2024) [DermNet®].
Why does a thinning subcutaneous fat layer leave superficial blood vessels vulnerable to rupture?
A thinning subcutaneous fat layer leaves superficial blood vessels vulnerable to rupture because it removes part of the soft support beneath the dermis. Small vessels are forced to tolerate more direct mechanical stress during minor trauma.
Bruising occurs when small capillaries and venules sustain physical damage, causing them to leak blood into the surrounding tissue. When deep padding remains healthy, these vessels ride safely atop a forgiving biological mattress.
This type of structural bruising represents a localized architectural collapse rather than a bleeding disorder. As subcutaneous volume retreats, it combines with dermal atrophy and cumulative photodamage to weaken the vascular support framework.
Without this dual layer of reinforcement, the capillaries are structurally stranded. Chronic photoaging explicitly triggers this dermal atrophy and collagen degradation. This loss of vascular support forces the vessels to endure greater mechanical stress (StatPearls, 2023) [NCBI].
| Skin State | Structural Feature | Mechanical Meaning | Bruising Result |
|---|---|---|---|
| Youthful or well-supported skin | Better dermal collagen support and fuller subcutaneous cushioning | Impact force spreads across a wider tissue area | Minor bumps are less likely to rupture superficial vessels |
| Photoaged thin skin | Dermal atrophy, collagen degradation, and reduced vascular support | Vessels lose structural reinforcement | Minor trauma can produce purple macules or ecchymoses |
| Very thin forearm/dorsal hand skin | Less padding and frequent sun exposure | Small vessels sit in a more fragile tissue environment | Actinic/senile purpura becomes more likely |
| Medication-amplified fragile skin | Corticosteroids, anticoagulants, aspirin, clopidogrel, or warfarin | Skin support or clotting response may be reduced | Bruises may appear more easily or persist visually |
What clinical signs suggest bruising from age-related skin and hypodermal thinning?
Clinical signs that suggest bruising from age-related skin and hypodermal thinning include recurrent dark purple patches on the backs of the hands or extensor forearms. These typically appear after minor trauma or pressure.
In dermatology, this presentation is diagnosed under overlapping terminologies like senile purpura or actinic purpura. Despite varying names, they describe the same benign condition caused by severe cutaneous and hypodermal atrophy.
Clinical authorities describe senile purpura as recurrent purple ecchymoses located on the extensor forearms (DermNetNZ, 2024) [DermNet®]. These vivid patches frequently transition into a persistent brown discoloration caused by residual hemosiderin deposits (MSD Manuals, 2023) [MSD Manuals].
Identifying these distinct purple macules alongside sun-damaged skin supports a benign structural diagnosis. Actinic purpura is a clinical diagnosis, but any rapid or escalating bruising patterns must be carefully reviewed by a physician.
| Sign | What It Suggests | Writer Note |
|---|---|---|
| Flat purple patches | Blood has leaked into superficial skin tissue | Use “macules,” “patches,” or “ecchymoses” |
| Back of hands and extensor forearms | Common pattern of actinic/senile purpura | Cite DermNet, StatPearls, or MSD Manual |
| Minor or unnoticed trauma | Fragile vessels can rupture with small impacts | Avoid implying trauma is always remembered |
| Brownish staining after purple fades | Hemosiderin can remain after red blood cell breakdown | Cite MSD Manual or DermNet |
| Thin, inelastic, sun-damaged surrounding skin | Supports the photoaging mechanism | Do not call this a blood disease by default |
Which medications and habits can worsen bruising linked to depleted hypodermal support?
Medications and habits can worsen bruising linked to depleted hypodermal support by weakening skin structure, reducing vascular support, or increasing bleeding visibility. Chronic exposure to systemic or potent topical corticosteroids is directly associated with severe skin thinning.
Corticosteroid exposure strips away remaining matrix proteins and worsens the skin’s mechanical fragility. Conversely, anticoagulants and antiplatelet drugs inhibit the body’s clotting cascade rather than destroying collagen.
When a less supported capillary ruptures upon minor impact, these blood-thinning medications simply make the leaked blood more visible or persistent. Dermatological authorities consistently list corticosteroids, warfarin, and aspirin as primary exacerbating factors (DermNetNZ, 2024; MSD Manuals, 2023) [DermNet®].
It is an important medical safety point that patients do not abruptly stop prescribed blood thinners out of cosmetic concern. Any anxieties regarding medication-amplified skin fragility must be reviewed with a prescribing clinician.
When should easy bruising from thin skin be checked by a healthcare professional?
Easy bruising from thin skin should be checked by a healthcare professional when bruises are sudden, frequent, unusually large, painful, or unexplained. Bleeding elsewhere or bruising soon after starting a new medication also requires evaluation.
Localized actinic purpura on sun-exposed forearms is often a benign sign of aging. However, patients must never casually dismiss severe vascular symptoms. Easy bruising can occasionally act as an early harbinger for a clinically important bleeding disorder.
Prominent medical institutions advocate a cautious approach to evaluating unexpected dermal bleeding. The threshold for seeking medical evaluation drops significantly if bruising departs from the typical pattern or presents on unexposed areas like the trunk.
To safely navigate the distinction between benign structural failure and a systemic condition, patients should rely on clinical warning signs. A medical red flags checklist helps identify dangerous hematological conditions swiftly (Mayo Clinic, 2023) [Mayo Clinic].
Medical Red Flags Checklist
What myths should be avoided when trying to fix easy bruising linked to subcutaneous fat loss?
Myths to avoid when trying to fix easy bruising linked to subcutaneous fat loss include the belief that iron supplements rebuild deep padding, that heavy moisturizers restore hypodermal volume, or that every purple bruise signals a dangerous blood disorder.
Misinterpreting the anatomy of aging skin frequently drives patients toward ineffective interventions. For example, iron supplementation is exclusively indicated when a clinical iron deficiency is confirmed via blood tests. It will not restore deteriorated hypodermal support.
Similarly, applying emollients is useful for mitigating epidermal dryness and preventing barrier water loss. However, these creams cannot penetrate deep enough to rebuild lost subcutaneous fat lobules or fortify fibrous septae.
Overinterpreting age-related purpura creates unnecessary anxiety. Believing that all dark purple bruises guarantee a bleeding disorder ignores the simple mechanics of less supported vessels. Reassuring patients that actinic purpura is largely benign remains a vital component of care.
| Myth | Reality |
|---|---|
| “Iron supplements rebuild thin skin.” | Iron can treat iron deficiency when diagnosed, but it does not restore lost hypodermal padding. |
| “Heavy moisturizer can rebuild subcutaneous fat.” | Moisturizers can improve surface dryness, but they do not replace deep adipose tissue. |
| “All purple bruises mean a blood disease.” | Actinic/senile purpura is often benign, but unusual bruising patterns still need evaluation. |
| “Vitamin K or Arnica cures thin-skin bruising.” | These ingredients may be used as adjuncts, but they do not rebuild the hypodermis or remove the need for protection. |
| “Stopping blood thinners will fix bruising.” | Prescribed anticoagulants should never be stopped without a clinician’s instruction. |
Which clinical or topical strategies may help protect skin with diminished subcutaneous cushioning?
Clinical or topical strategies may help protect skin with diminished subcutaneous cushioning by strengthening the visible skin envelope, reducing further photodamage, and adding external protection against minor trauma.
It is medically crucial to clarify that no over-the-counter topical cream can rebuild lost hypodermal fat. Non-surgical aesthetic management depends mainly on maximizing the health of the remaining dermis and shielding this vulnerable tissue from external insults.
Regimens utilizing actives like retinoids and vitamin C optimize remaining collagen synthesis rather than functioning as fat-restoration treatments. Long-term management of actinic purpura emphasizes patient education and rigorous photoprotection (StatPearls, 2023) [NCBI].
Clinical guidelines overwhelmingly emphasize diligent sun protection alongside the daily use of protective clothing to serve as a missing mechanical buffer (DermNetNZ, 2024) [DermNet®]. Implementing impact-resistant protective sleeves represents a direct, effective strategy.
How can topical retinoids and vitamin C support fragile, photoaged skin?
Topical retinoids and vitamin C may support fragile, photoaged skin by improving epidermal and dermal resilience. Retinoids encourage fibroblasts to spin new, healthier collagen fibers to thicken the superficial envelope over time.
Vitamin C functions as a critical antioxidant that neutralizes free-radical damage and helps defend vascular walls. However, fragile elderly skin possesses a compromised barrier that may become irritated.
Neither active ingredient should be marketed as a rapid cure for structural bruising. Introducing these actives should always be executed under clinician-guided supervision to ensure safety and tolerance.
What role do Vitamin K, Arnica, and physical barriers play in bruise management?
Vitamin K, Arnica, and physical barriers play supportive roles in bruise management, but physical protection is the most direct strategy. While Vitamin K and Arnica are sometimes used as adjunctive bruise-care ingredients, their clinical evidence remains limited.
Defending the forearms with long sleeves and impact-resistant clothing serves as a highly effective external shock absorber. By reducing friction during daily tasks, patients can reduce the mechanical shear forces that instigate purpura.
What daily checklist helps manage bruising risk from structural fat depletion?
A daily checklist helps manage bruising risk from structural fat depletion by combining medical review, sun protection, friction reduction, gentle skin care, and physical barriers. Implementing a realistic, safety-oriented routine empowers patients to actively defend their fragile skin from daily mechanical stressors.
Daily Tissue-Protection Checklist
Clinical Key Takeaway
Actinic purpura on the hands and forearms is predominantly a structural issue driven by severe hypodermal depletion and cumulative photodamage. While topical supports may incrementally enhance remaining dermal resilience, the most effective management strategy depends mainly on consistent physical protection—acting as an external shock absorber—and routine medical evaluation of exacerbating medications.
Quick Answers About Thin-Skin Bruising
Why does skin bruise more easily with age?
Skin bruises more easily with age because the protective subcutaneous fat layer thins, and dermal collagen degrades. This loss of structural cushioning leaves superficial blood vessels highly vulnerable to minor mechanical trauma.
What is actinic purpura?
Actinic purpura is a benign clinical condition characterized by recurrent dark purple patches, typically on the sun-damaged dorsal hands and extensor forearms, resulting directly from severe cutaneous and hypodermal atrophy.
Can heavy moisturizers rebuild thinning skin?
No. While heavy moisturizers effectively treat epidermal dryness and prevent barrier water loss, they cannot penetrate deep enough to physically rebuild lost subcutaneous fat lobules or fortify the underlying dermal collagen.
Why do blood thinners make bruises look worse?
Anticoagulants and antiplatelet drugs inhibit the body’s clotting cascade. When a fragile, unsupported capillary ruptures upon minor impact, these medications allow more blood to leak into the tissue before clotting, making the bruise larger and more persistent.
When should easy bruising be evaluated by a doctor?
Easy bruising should be evaluated if it appears suddenly, frequently, without any trauma, on unexposed areas like the trunk, or is accompanied by other bleeding symptoms, as this could indicate an underlying systemic or hematological condition.
Conclusion
Reduced hypodermal thickness increases bruising risk by weakening the skin’s deep cushioning system. Less supported, superficial blood vessels rupture under minimal pressure, resulting in the classic presentation of recurrent structural bruising.
Recognizing the distinct visual hallmarks of actinic and senile purpura reassures patients. Vivid macules concentrated on sun-damaged dorsal hands and extensor forearms are often a benign sign of aging.
At SkinKeeps, we explain skin aging through evidence-based dermatology. By recognizing the mechanical deficit responsible for these lesions, individuals can effectively guard their fragile tissues with confidence and calm.