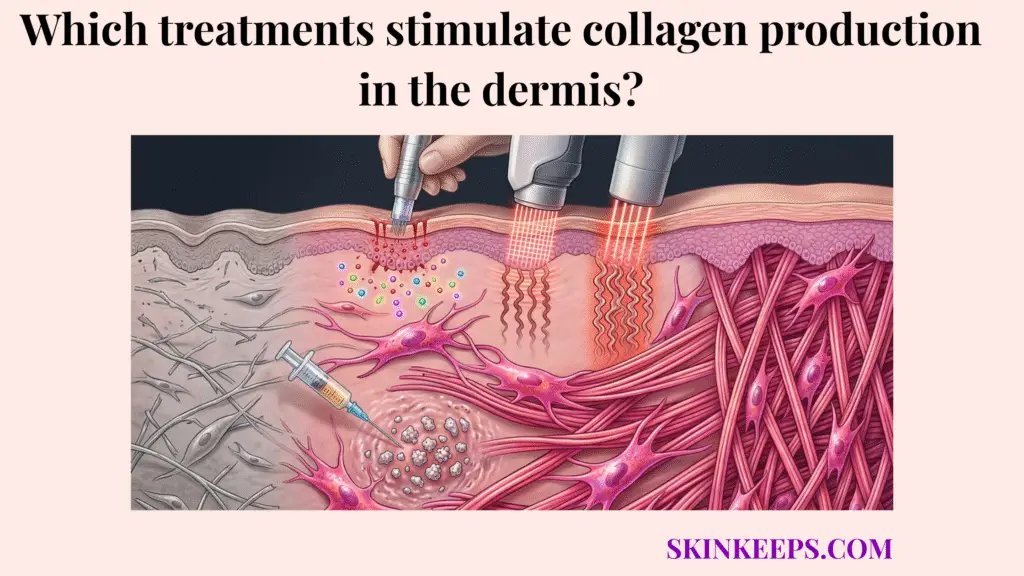
The main treatments that stimulate collagen production in the dermis include topical retinoids, vitamin C–based antioxidant support, microneedling, fractional laser procedures, radiofrequency-based treatments, and certain biostimulatory injectables. These treatments work by either improving fibroblast signaling, reducing collagen-suppressing damage, or triggering controlled repair pathways that lead to new collagen formation.
Not every anti-aging treatment truly stimulates collagen. Some ingredients focus purely on surface hydration, while others merely protect existing collagen from environmental breakdown. A true stimulator must physically or chemically compel the skin’s deep cellular machinery to synthesize fresh matrix proteins.
Understanding which treatments stimulate dermal collagen production makes it easier to navigate photoaging therapies. By separating topical signaling from procedural remodeling, setting realistic timelines, and matching treatment intensity to skin damage, we can isolate exactly what works to restore dermal firmness.
What is the biological baseline for how treatments stimulate dermal collagen production?
The biological baseline is that dermal collagen is produced mainly by fibroblasts, and treatments stimulate dermal collagen production when they activate fibroblast signaling, trigger repair pathways, or induce controlled wound-healing cascades that lead to gradual matrix rebuilding. New collagen does not appear immediately because synthesis, organization, and remodeling take time.
Fibroblasts are the specialized cells housed deep within the dermis responsible for building the extracellular matrix. If a treatment does not somehow engage these specific cells, it cannot produce neocollagenesis (the formation of new collagen).
When activated, fibroblasts generate and secrete the precursors required to weave new, tight structural fibers. The skin interprets this stimulation as a command to rebuild, reinforcing areas depleted by chronological aging or collagen density loss.
Biological Pathway
- Target cell → fibroblast
- Main process → signaling or controlled repair activation
- Result → new collagen synthesis and gradual dermal remodeling
Which topical treatments stimulate dermal collagen production most directly?
Among topical treatments, retinoids stimulate dermal collagen production most directly and with the strongest evidence. Reviews of photoaging therapy consistently position topical tretinoin as a gold-standard topical anti-aging agent because it improves epidermal differentiation and supports collagen-related dermal change.
While many cosmetic ingredients make vast claims about rebuilding the skin, prescription retinoids possess decades of histologic proof showing their ability to traverse the epidermis and actively alter dermal behavior.
This class of topicals acts as a true biological communicator, telling sluggish fibroblasts to resume production.
How do retinoids stimulate dermal collagen production?
Retinoids stimulate dermal collagen production by improving skin-signaling pathways linked to repair and by normalizing photoaged skin behavior. Understanding how retinoids influence dermal fibroblast activity clarifies why they support collagen-related remodeling over time. Histologic and systematic-review evidence supports tretinoin as one of the most reliable topical options for photodamaged skin.
By binding to specific nuclear receptors within skin cells, retinoids actively suppress the destructive enzymes (MMPs) that degrade collagen while simultaneously increasing the expression of procollagen genes.
Griffiths et al. (1993) found that collagen I formation was 56% lower in photodamaged skin than in protected skin, and that topical tretinoin treatment produced an 80% increase in collagen I formation, while vehicle treatment produced a 14% decrease. This is one of the clearest quantitative anchors for topical collagen stimulation [PubMed] [PMC].
How do prescription retinoids compare with cosmetic retinol in treatments that stimulate dermal collagen production?
Prescription retinoids usually stimulate dermal collagen production more strongly and more predictably than cosmetic retinol, although retinol can still contribute to milder long-term support depending on formulation, stability, tolerance, and consistency.
Because retinol must undergo a two-step conversion process within the skin to become biologically active retinoic acid, a significant portion of its potency is inherently lost. Prescription tretinoin is already active and binds directly to receptors.
Therefore, while retinol provides an excellent, less irritating entry point, it remains a milder, secondary stimulator compared to prescription-strength intervention.
How do antioxidant treatments stimulate dermal collagen production indirectly?
Antioxidant treatments stimulate dermal collagen production more indirectly by improving the biochemical environment in which fibroblasts function. Vitamin C is the clearest example because fibroblasts have an absolute dependence on vitamin C for collagen synthesis, and antioxidants also reduce oxidative stress that suppresses collagen-supportive activity.
If the dermis is constantly battling free radicals generated by UV radiation, fibroblasts remain suppressed and focused on emergency repair. Antioxidants act as biological shields that neutralize this chaos.
Pullar et al. (2017) note that skin fibroblasts have an absolute dependence on vitamin C for collagen synthesis, and topical vitamin C literature describes increased type I collagen and better collagen stability in photodamaged skin [PMC] [PMC]. Thus, vitamin C is best framed as heavily collagen-supportive, not as an instant structural replacement.
How do peptide-based treatments stimulate dermal collagen production?
Peptide-based treatments stimulate dermal collagen production more subtly by acting as repair-related signaling molecules in the skin, but their effects are usually milder and more formulation-dependent than retinoids or procedures. Recent reviews describe peptides as promising collagen-supportive ingredients rather than the strongest standalone collagen-building tools.
Certain specific signaling peptides mimic the fragments of broken collagen, theoretically tricking the skin into believing a structural breakdown has occurred, which prompts a mild synthetic response.
While conceptually elegant, peptide molecules are large and struggle to penetrate the epidermis effectively. Pintea et al. (2025) note that peptides are emerging candidates for the prevention and treatment of skin aging, positioning them as excellent adjuncts rather than primary heavy-lifters [PMC].
Which in-office treatments stimulate dermal collagen production through controlled injury?
The main in-office treatments that stimulate dermal collagen production through controlled injury are microneedling, fractional laser procedures, and radiofrequency-based treatments. These approaches work by creating targeted mechanical or thermal stress that activates wound-healing and remodeling pathways leading to new collagen formation over time.
This entire class of treatments exploits the skin’s biological emergency response. When the dermis is physically or thermally injured, it instantly deploys growth factors and active fibroblasts to patch the defect, resulting in a denser, fresher matrix.
How does microneedling stimulate dermal collagen production?
Microneedling stimulates dermal collagen production by creating controlled micro-injury that triggers wound-healing pathways and collagen induction without the same degree of epidermal ablation seen in more aggressive procedures. Understanding how microneedling triggers collagen synthesis in the dermis reveals why this process is widely described as collagen induction therapy.
By piercing the tissue with tiny needles, it creates thousands of microscopic puncture channels. The body responds to this perceived trauma by rushing blood, nutrients, and repair cells to the area. Jaiswal et al. (2024) describe microneedling as an established technique for promoting dermal rejuvenation, classifying it as a moderate-remodeling procedure with manageable downtime [PMC].
How do fractional lasers stimulate dermal collagen production?
Fractional lasers stimulate dermal collagen production by creating targeted columns of ablative or non-ablative thermal injury that trigger stronger remodeling and neocollagenesis than many topical approaches. Fractional resurfacing literature consistently links these treatments to robust wound-healing activation and collagen remodeling.
Unlike fully ablative lasers that burn away the entire surface, fractional lasers leave healthy tissue intact around each microscopic burn column. This allows for profound deep-tissue heat stress while maintaining a safer, faster recovery profile. Borges et al. (2020) emphasize that fractional laser resurfacing treats photoaging by directly promoting neocollagenesis [PMC].
How do radiofrequency treatments stimulate dermal collagen production?
Radiofrequency treatments stimulate dermal collagen production by heating dermal tissue in a controlled way that promotes collagen remodeling and tightening-related repair responses. When evaluating which energy-based devices tighten dermal tissue, these treatments serve as primary options, though their exact effect depends heavily on device type, depth, energy delivery, and whether the treatment is noninvasive, microneedling-assisted, or fractional.
Thermal energy causes immediate contraction of existing collagen fibers while simultaneously provoking a delayed, secondary healing response. Zhang et al. (2025) reported that skin-texture improvement ranged from 71% to 100% across included studies and skin-firmness improvement from 52.9% to 100%, though these figures reflect heterogeneous RF devices and should be used as broad context rather than a universal guarantee [PMC].
Which injectable treatments stimulate dermal collagen production from within the dermis?
Certain injectable treatments stimulate dermal collagen production from within by creating a biostimulatory response rather than only supplying temporary volume. The best-known examples are calcium hydroxylapatite (CaHA) and poly-L-lactic acid (PLLA), which are repeatedly described as biostimulatory injectables in dermatologic and aesthetic literature.
Unlike traditional hyaluronic acid fillers that simply occupy space to push the skin up, biostimulators provoke a mild inflammatory reaction. The injected microspheres act as foreign bodies that the skin attempts to encapsulate with fresh, dense collagen.
Amiri et al. (2023) show that histologic work on CaHA demonstrates a significant increase in newly formed type III collagen compared with control tissue, proving that this category actively modifies dermal structure rather than just inflating it [PMC] [PMC].
How do topical and procedural treatments compare in how they stimulate dermal collagen production?
Topical and procedural treatments compare differently because topicals usually provide slower, lower-intensity, signaling-based stimulation, while procedures tend to trigger stronger remodeling by mechanical or thermal injury, often with more downtime and greater short-term intensity.
Choosing between them is a matter of calculating expected results against acceptable downtime and financial investment.
| Treatment class | Main mechanism | Relative collagen stimulation strength | Downtime level |
|---|---|---|---|
| Retinoids | Signaling-based dermal support | Moderate | Low to moderate |
| Vitamin C / Antioxidants | Protective and supportive | Mild to moderate | Low |
| Peptides | Signaling support | Mild | Low |
| Microneedling | Controlled micro-injury | Moderate | Mild |
| Fractional lasers | Stronger controlled remodeling | Higher | Moderate to higher |
| Radiofrequency | Thermal remodeling | Moderate to higher | Mild to moderate |
| Biostimulatory injectables | Internal fibroblast stimulation | Moderate to higher | Variable |
How long do treatments stimulate dermal collagen production before results become visible?
Treatments stimulate dermal collagen production on a delayed timeline because new collagen must be synthesized, organized, and remodeled gradually before visible firmness improves. Early changes may reflect hydration, edema, or transient inflammation, while true structural remodeling usually unfolds over weeks to months.
You cannot speed up biology. A procedure may take 30 minutes to perform, but the fibroblasts require months to lay down the collagen fibers tightly enough to visibly alter skin tension.
What limits the effect of treatments that stimulate dermal collagen production?
The effect of collagen-stimulating treatments is limited by fibroblast responsiveness, baseline photoaging severity, ongoing UV exposure, inflammation, metabolic health, and the biological ceiling of the tissue itself. Even strong procedures do not create unlimited collagen gain when the repair environment is poor or the damage is advanced.
If an older patient with heavy sun damage and thin, fragile tissue undergoes fractional laser therapy, their sluggish fibroblasts simply cannot produce the same volume of robust collagen as a younger patient with high metabolic energy.
Which treatments stimulate dermal collagen production best for mild versus advanced photoaging?
The treatments that stimulate dermal collagen production best depend on severity: milder photoaging often fits retinoids, antioxidants, and lower-intensity procedures such as microneedling, while more advanced photoaging often needs stronger remodeling strategies such as fractional lasers, radiofrequency-based procedures, or biostimulatory injectables.
Mild damage requires preservation and signaling support. Severe damage requires heavy architectural reconstruction.
What supportive habits improve the results of treatments that stimulate dermal collagen production?
Supportive habits improve collagen-building outcomes because new collagen remains vulnerable to ongoing UV damage, inflammation, poor tolerance, smoking-related vascular stress, and inconsistent treatment habits. Daily broad-spectrum sunscreen protection is the single most important supportive behavior because UV exposure degrades collagen and undermines remodeling gains.
If you undergo expensive collagen induction therapy but refuse to wear SPF, ultraviolet radiation will rapidly unleash MMP enzymes to chop up the fresh collagen your skin just fought to synthesize.
What steps can you take today if you want treatments that stimulate dermal collagen production to work better?
The best day-to-day way to improve collagen-stimulating treatment outcomes is to combine daily broad-spectrum sun protection, a proven collagen-supportive topical such as a retinoid when appropriate, and procedure choices matched to severity and downtime tolerance. Progress should be measured over months, not days.
Final Execution Checklist
What are the key summary facts about treatments that stimulate dermal collagen production?
The key summary facts are that retinoids are the strongest evidence-based topical collagen stimulators, vitamin C and antioxidants are more supportive and protective, and microneedling, fractional lasers, radiofrequency, and some biostimulatory injectables stimulate collagen through stronger repair or remodeling pathways. True dermal collagen gain remains gradual and depends on fibroblast function, consistency, and UV control.
Summary Checklist
Quick Answers About Treatments That Stimulate Dermal Collagen Production
Which treatment stimulates dermal collagen production most strongly on the topical side?
Among topicals, tretinoin and other retinoids have the strongest evidence for stimulating dermal collagen production. They work more directly than most cosmetic actives because they influence signaling pathways tied to repair and dermal remodeling.
Does vitamin C really stimulate collagen, or does it just protect it?
Vitamin C does both, but it is usually better framed as collagen-supportive and antioxidant rather than equally direct to retinoids or procedures. Fibroblasts depend on vitamin C for collagen synthesis, but the practical effect is more supportive than high-intensity remodeling.
Are peptides strong collagen stimulators?
Usually not at the same level as retinoids or procedures. Peptides may support repair-related signaling and collagen-friendly behavior, but results are more formulation-dependent and generally milder.
Does microneedling really create new collagen?
Yes, that is the core rationale behind collagen induction therapy. Microneedling creates controlled micro-injury that activates wound-healing pathways associated with gradual neocollagenesis.
Are fractional lasers stronger than microneedling for collagen remodeling?
Generally yes. Fractional lasers usually trigger stronger remodeling because they create more intense controlled thermal or ablative columns, but they also tend to come with more downtime and intensity than microneedling.
Can radiofrequency tighten skin by stimulating collagen?
Yes, many RF-based treatments aim to stimulate collagen remodeling through controlled dermal heating. The exact effect depends heavily on the device, depth, and treatment design, so RF should be treated as a category rather than a single uniform result.
Which injectables stimulate collagen instead of just filling space?
The best-known biostimulatory injectables are calcium hydroxylapatite (CaHA) and poly-L-lactic acid (PLLA). They are used because they can trigger fibroblast-driven collagen response rather than acting only as passive volume fillers.
How long does it take to see real collagen results?
Real collagen remodeling usually takes weeks to months, not days. Early post-treatment changes may reflect swelling, hydration, or inflammation, while true dermal remodeling takes longer to organize visibly.
What ruins collagen-building progress the fastest?
Ongoing UV exposure is one of the biggest ways to undermine collagen-building progress because it degrades collagen and counteracts new matrix formation. Inconsistency, excessive irritation, and poor recovery habits also reduce results.
What is the best starting strategy for mild photoaging?
For mild photoaging, the most sensible starting strategy is usually daily broad-spectrum sunscreen, a retinoid if appropriate, and possibly a supportive antioxidant such as vitamin C, with procedures considered later if needed.
Conclusion
In conclusion, treatments stimulate dermal collagen production through three main pathways: direct signaling support such as retinoids, biochemical support such as vitamin C and antioxidants, and controlled remodeling or injury-based pathways such as microneedling, lasers, radiofrequency, and biostimulatory injectables. The best results come from matching treatment intensity to damage severity and protecting new collagen long enough for real remodeling to happen.
Appropriate stimulation method, a realistic time horizon, and strong collagen protection ensure that fibroblast-driven remodeling improves and that structural skin change becomes more believable and sustainable over time.